


“Formal complaints are managed by the Complaints team who are responsible for ensuring that all responses to formal complaints contain an acknowledgement, an apology, an explanation of the facts and any changes being made as a result of the complaint” Moorfields: Being Open and Duty of Candour
[AI Overview]
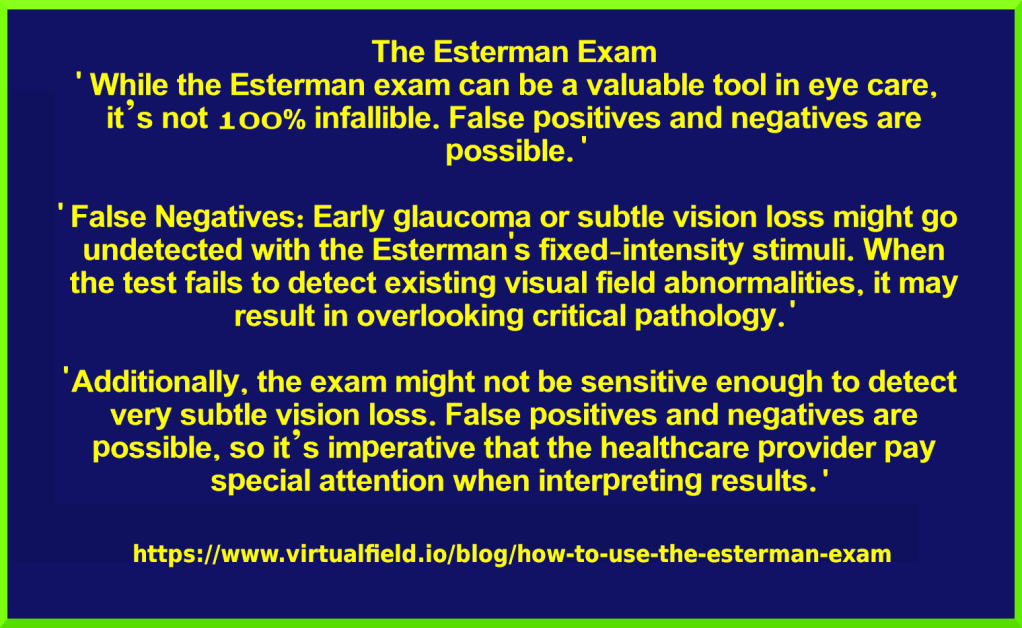
The Esterman binocular visual field test, used for driving assessments, has significant limitations, including potential for false results due to poor patient cooperation, inability to measure fixational stability, and low sensitivity to subtle, early, or central vision loss. It is a suprathreshold test which may not accurately reflect real-world driving functionality
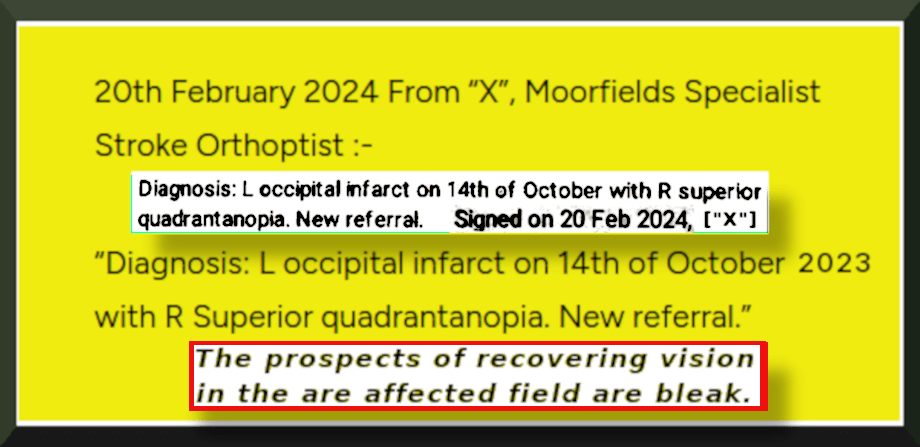
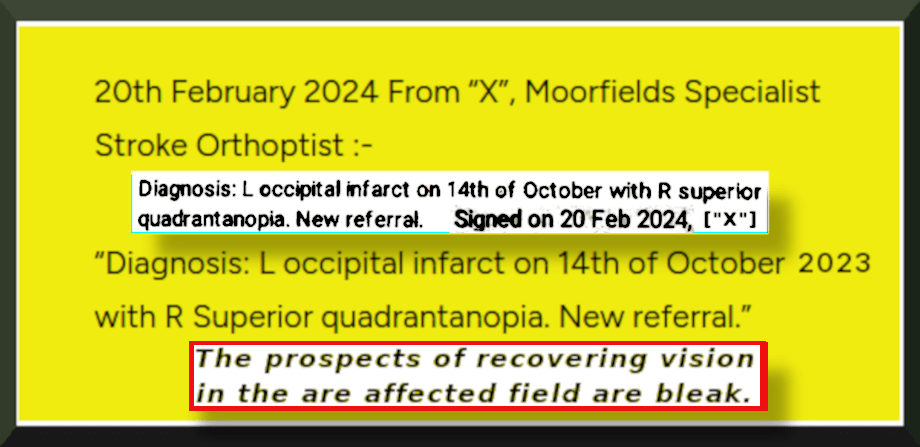
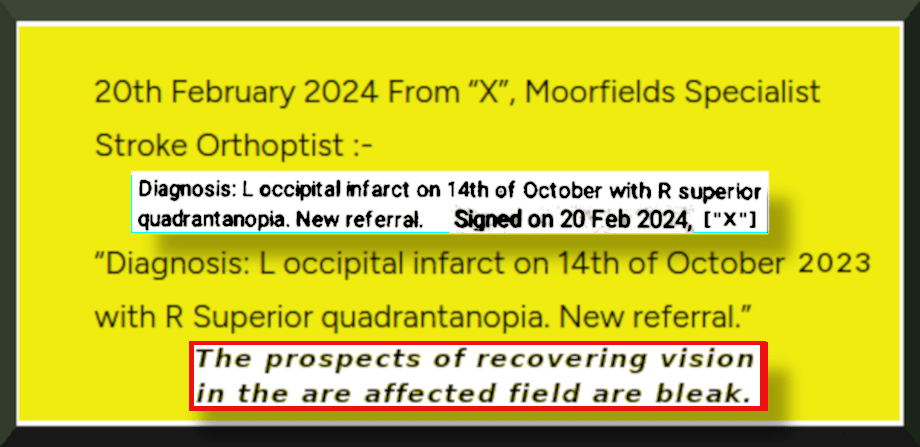
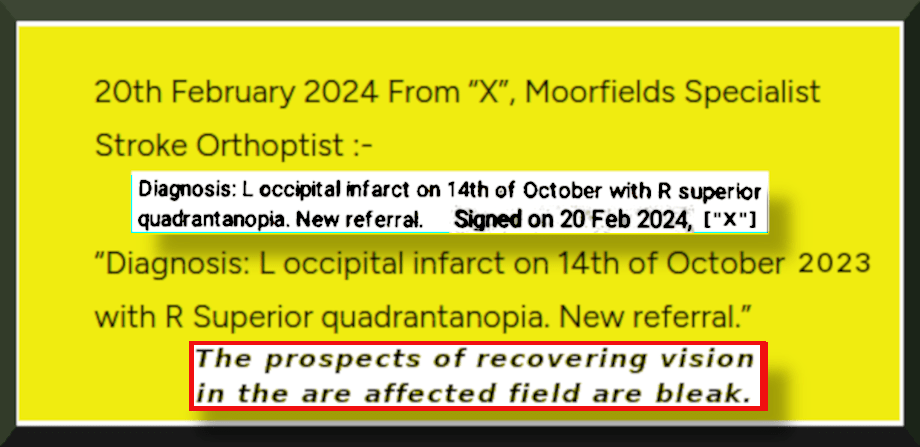
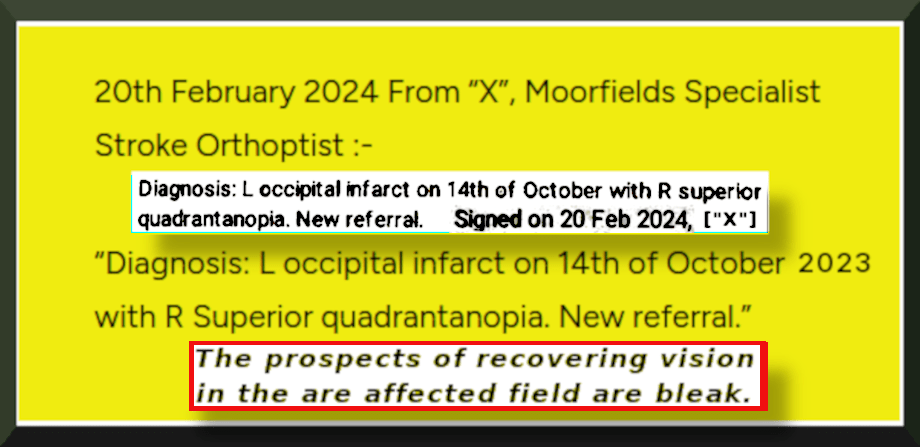
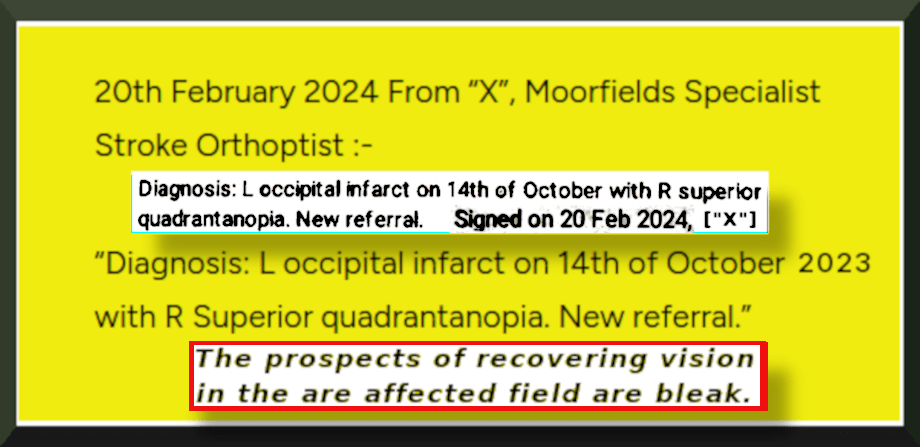
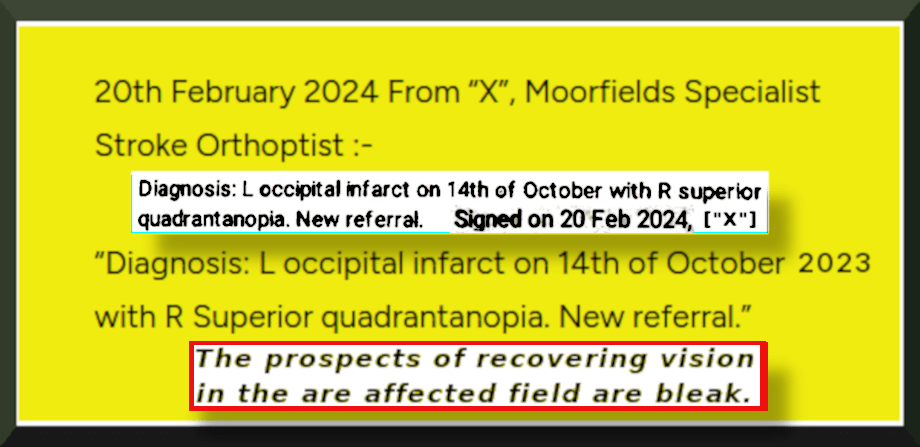
The prospects of recovering vision in the affected field are bleak. Occasionally, patients will spontaneously recover vision in the affected field within the first three months after the brain injury; however, vision loss remaining after this period of spontaneous recovery is traditionally thought to be permanent, certain companies now claim to be able to induce recovery of vision after this three-month period. https://en.wikipedia.org/wiki/Quadrantanopia
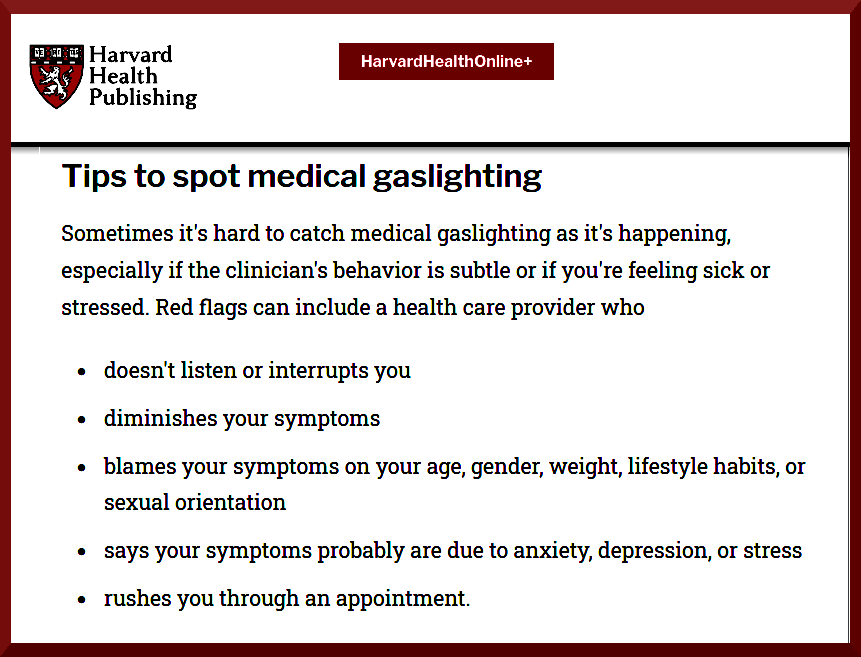
https://www.health.harvard.edu/staying-healthy/what-to-do-about-medical-gaslighting
” … we define “medical gaslighting” as the psychological and institutional process that naturalizes the diminution of those who are testimonially disempowered within the context of the medical institution, and in their relationship with those who have authority to legitimize the patient’s illness experience“.
“Medical gaslighting as a mechanism for medical trauma: case studies and analysis“
Devora Shapiro, Anna Hayburn, Current Psychology (2024) 43:34747–34760 https://doi.org/10.1007/s12144-024-06935-0
“The amount of energy needed to refute bullshit is an order of magnitude bigger than that needed to produce it“
Brandolini’s law: https://en.wikipedia.org/wiki/Brandolini%27s_law

November 20th 2023: “Dear [GP Practice] Please Find attached … optician report from 12/11/2023. [ed. requested by GP Practice before any referral could be made] I am very troubled by what I understand to be homonymous hemianopia. This follows cerebral infarction of 12/10/2023 ….etc.” [12th November 2023 = “eye check“]
November 22nd 2023: Moorfields Eye Hospital: Orthoptics appointment booked: Thu 14th Mar at 9.00am at Moorfields at St Georges Hospital
On the 7th of May 2024 My Complaint Document was sent via Royal Mail Signed For 1st Class to Complaints at St George’s Hospital Tooting arriving 8th May. Following delays and failures, I then sent a copy directly by email to Dr Martin Kuper, who was then the CEO at Moorfields, on 24th May 2024:
“I am wondering if you may be able to help” …… “Please consider this as a formal complaint.
I attended Moorfields Eye Hospital at St George’s on Tuesday 30th April at 10am.
<>
I was seen by “X”.
At the very outset, I made it abundantly clear, that post stroke, I have a centrally situated blind spot.
“X” acknowledged this, and appeared to understand me, as if routinely familiar with the phenomenon.
Following a negative test, which I believe was insensitive, I was subjected to about 15 minutes of rude interruption by “X”, at a rate of about one rude interruption per minute.
“X” appeared intent on heading off any evidence that might contradict the test result, and her apparent conviction of its’ infallibility.
Also within this period, I was told my vision was “OK” on about four separate occasions, “perfect” on about three separate occasions, “no problem” on about three other occasions, and that the stroke had not affected my visual pathway.
On two occasions I had to request that “X” actually listen to what I had to say.
At one point, I had thought about stepping into the corridor in order to find a witness.
I gave precise, easy to grasp examples of the hole in my vision, presenting “X” with about eight different scenarios, where the defect is very obvious to me, including how cars passing by while I stand at the kerb, can appear (out of nowhere as it were) and disappear (similarly).
I finally mentioned to “X” that I lose objects at home because I can’t see properly.
This is another very distressing problem.
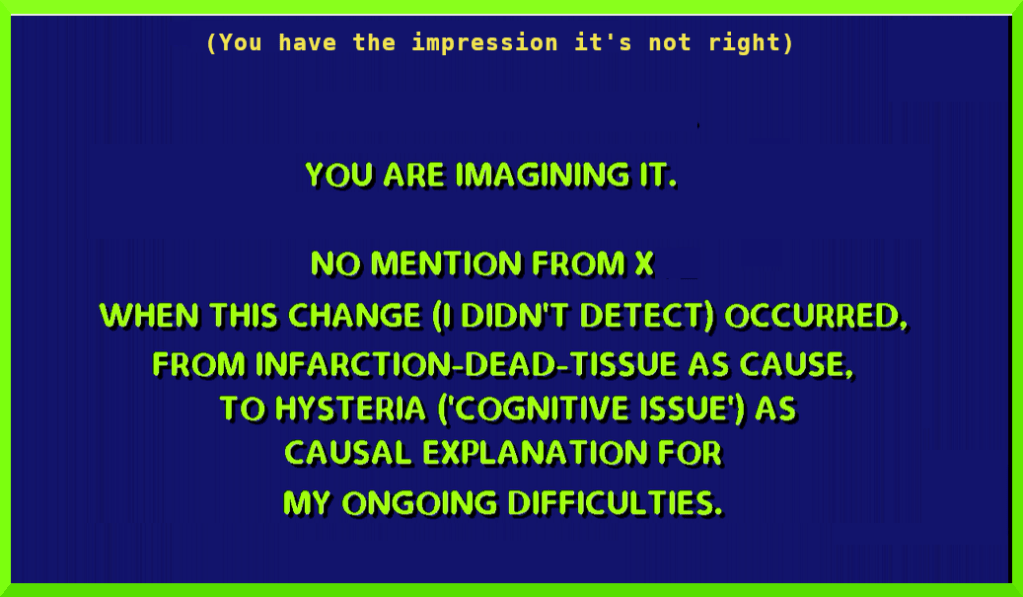
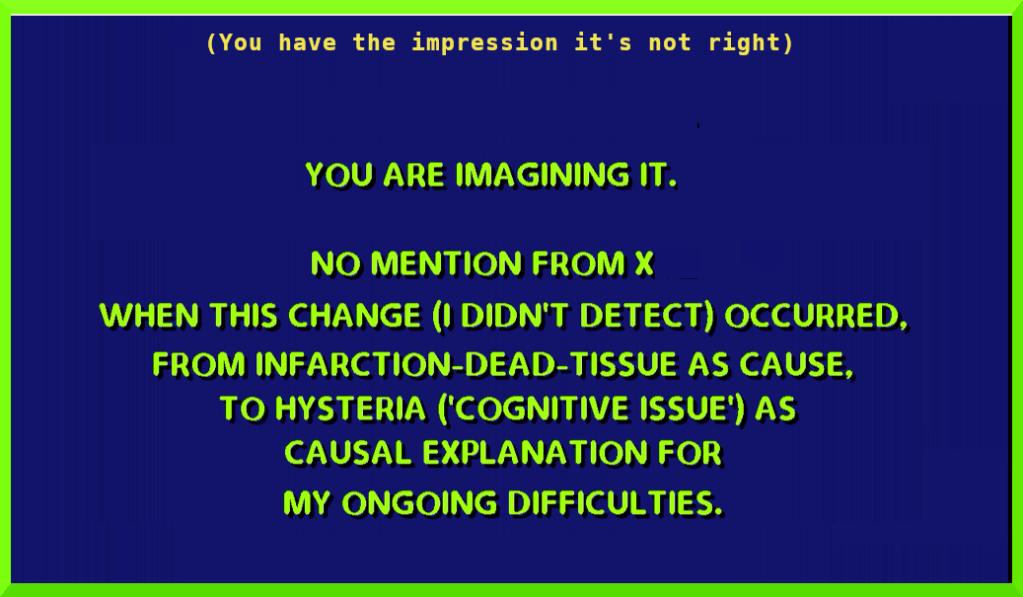
The chilling response from “X” was: “You can see well sir …. it’s a cognitive issue…. you have the impression it’s (ed. my VF defect) not right”
I had already mentioned to “X” that I thought the test was not refined enough to pick up the hole in the middle of my visual field.
The individual concerned was repeatedly disrespectful of the reality of my life, the reality of my distressing experiences, the reality of my symptoms, and was seemingly incapable of stopping and thinking rationally.
Some of the patronizing and disturbing behaviour “X” exhibited, bordered on the abusive, and at times “X” shouted at me from a very close range.
I was left with an intrusive visual problem on discharge from the St George’s Stroke Unit, on the 14th of October 2023.
For six months I have lived with a problem I am very familiar with indeed.
For six months I have been without any expert help on the issue.
There has been no change in the visual blind spot that intrudes into almost every aspect of my life.
Being a central blind spot, it does not take much imagination to understand the problems I encounter daily, some of which are dangerous.
During this appointment, the explanations and suggestions I received from “X” were frankly insulting.
For example, the visual deficit that I have the “impression” I am suffering from, should get better with glasses.
I have never used or felt the need for glasses.
There was no thoughtful or properly adequate interrogation of my situation.
There were only what appeared to be two rather chaotic and irrelevant office tests by “X”.
I understand that the scientific attitude requires humility, a willingness to accept criticism, plus a desire to eagerly revise your work where appropriate, to everyone’s best interest.
In “X”, I did not notice the hallmarks of a scientific attitude, so to speak.
I was shocked by the overbearing arrogance of this individual, who appeared to think that a test result (which may well be a false negative), somehow licensed her to harangue a member of public for the best part of twenty minutes.
I believe this needs serious and thoroughly independent investigation, and appropriate remedy.” [ends]

All comments and entries are In My Opinion

Some examples of this NHS Moorfields appointment: 30 April 2024
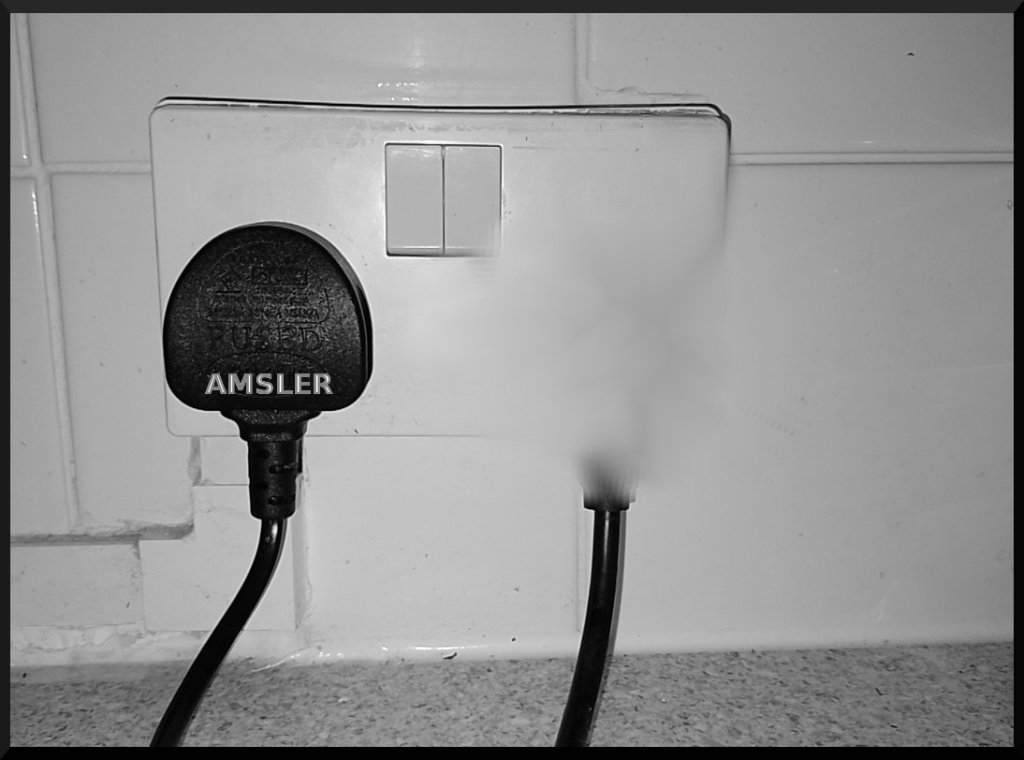
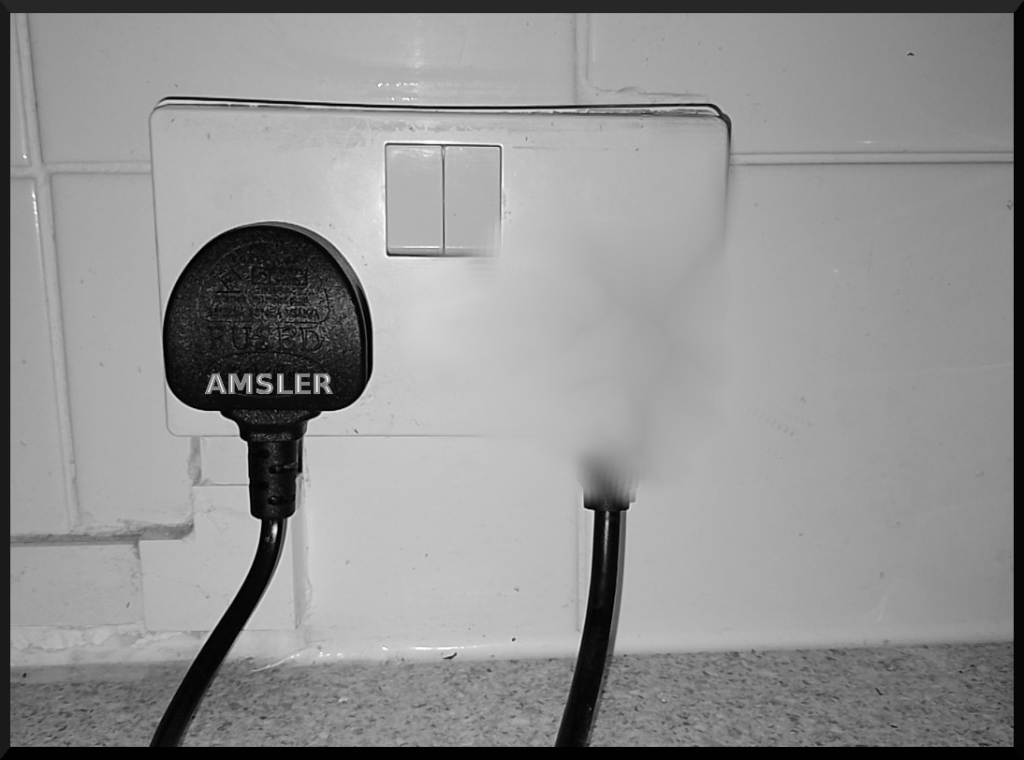
In part one, before the Esterman visual field test, I had used a double electrical socket with two plugs inserted (below -but not the original) which was usefully in view, as an example. “X” appeared to understand that when I looked to the left hand plug, the right hand one ‘disappeared’. (“X”) – “It disappears. It’s not double. OK … I repeated this just to be absolutely clear … (“X”) – OK. OK. That’s OK”.

Interrupting and talking over me, from the very outset of the second part of this interview (following a negative Esterman Test), the appointment proceeded roughly as follows: The Esterman test was described by “X” as “perfect”. “X” then said “So you told me that a now you’ve still a problem?”, and so I explained that the problem was ‘in the middle … *rather than …it’s … it’s*… ‘ as “X” hastily interrupted talking over me: “What do you mean in the middle? ‘Yeah … *it’s … it’s that* … So if you look at this one have you got the glasses?” (No) …. there followed some pointed sarcasm when I couldn’t catch what had been said next …. and then: “Can you see my face?” ‘Yes’. “Can you see the eyes?” ‘If I look to your right eye, you’ve only got one eye’ (repeating the essence of the earlier plug sequence). “Say again sorry” (as if this was now impossible). ‘If I look at your right eye, the other eye’s missing, it disappears… ‘ “But you see, the test is perfect” ….. ‘Say I’m looking at these two plugs‘ … “How many plugs do you see sir?” ‘If I look at the left hand one’ ....“Doesn’t matter which one, if you look in front of you how many now?” ‘If I look absolutely in front (obviously meaning straight ahead and centre between the two plugs) there’s the two’ ...“Sir sir, if you look at my face how many eyes do you see?” … ‘There’s the two‘...“So what is the problem?” contemptuously ….. I explain the situation to “X” for the fourth time… “But you see two eyes if you look at my face?” ‘If I look straight on yes’ ... “That’s OK“ ‘But not if I look if I look to the side’ .... “X” abruptly interrupted me making clear she was not in the slightest interested, having got ………. The Correct Answer.
*central ‘rather than‘ peripheral – ‘in the middle’
Brushing me aside, “X” scornfully announced that my visual field was “all right” and there was “no problem about” my visual field.





I came to this much anticipated appointment hoping for expert advice, and perhaps some wisdom, having come across little that was positive in connection with recovery from hemianopias, other than some remarkable claims about coloured lenses and carnivorous diets.
I considered walking out and engaging a witness, but realised that, in this particular instance, such action could be counterproductive.
Without any explanation, there followed an absurd and chaotic, subjective, impatient, bad-tempered office test, inappropriately peppered with “well-done” – “correct“- jibes, which, as some form of test, appeared to be hopelessly vulnerable to operator bias, self-deception, and manipulation.
Apparently my vision was “OK”, my “central vision” was “OK”, my peripheral vision was “OK”, and sounding exasperated, there was “No problem at all”. I again attempted to explain something of the reality of my situation (as in the above representations), but “X” butted in with the claim that I was “too focused on something” [meaning to the left hand side], and “You need to look with both eyes open normally”. Both eyes were of course open normally. Later, again raising her voice on this same point, and rather confusingly through her anger : “SO IS NOTHING DISAPPEARED THE SECOND EYE … THE TWO EYES ARE LIKE THE PLUG” … ‘the right one disappears’ I pointed out … “BECAUSE YOU ARE NOT PROBABLY CONCENTRATED ON THE OTHER EYE, YOU ARE FOCUSING ON ONE EYE” -incensed I’d once more tried to clarify a fact of the matter.
Victim-blaming and mockery in a health care setting behind closed doors, in a major NHS Teaching Hospital, was quite unexpected.
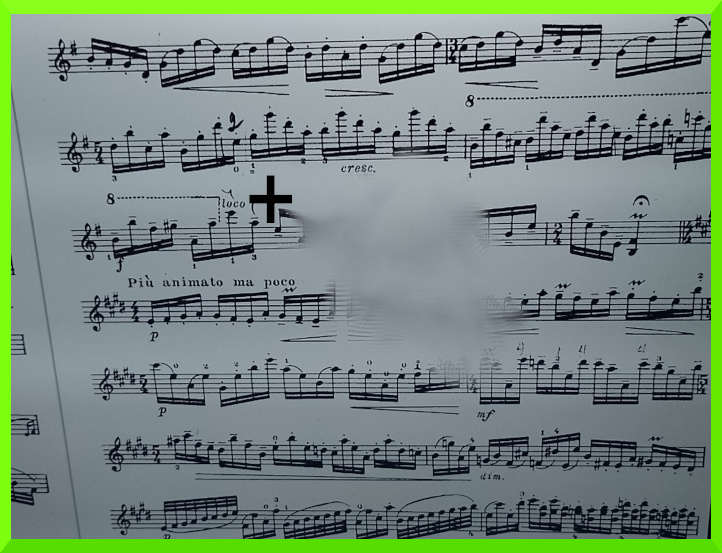
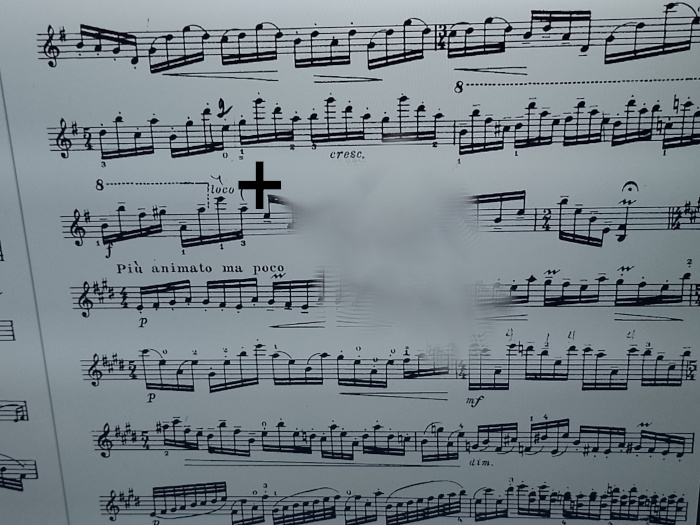
I continued with: “…say reading music…”, as an example, which I quickly regretted because it was easy to exploit. I explained, pointing at a bar-like segmented row on the computer screen ‘here’s a bar, but the next bar is missing’ – “Which next bar?”
After trying to explain the situation as best I could under these circumstances, being discouraged by the impatient “… yeah… yeah… yeah...” staccato accompaniment, “X” exclaimed “DO YOU USE THE GLASSES?” ‘No.’ “X” tried to convince me, “… maybe it would be better… WHY NOT?” to which I objected, with good reason, but was unable to go into much detail because of the inhospitable conditions. Without waiting for an answer, “X” then snapped at me: “HOW OLD ARE YOU NOW SIR?” … ‘How old?‘ … appalled by this incursion and the aggressive tone of someone who had my DoB in front of them “… HOW OLD ARE YOU?” <>..age supplied..<> “WHAT IS YOUR AGE?” <>..age supplied..<> “SO AT THIS AGE YOU NEVER USED THE GLASSES FOR DISTANCE” …’I’ve never used glasses‘ …. “CORRECT …. AT THIS AGE YOU SHOULD USE THE GLASSES FOR MUSIC AND FOR READING …”, pontificated “X” at full volume.
Trying to prevent any further misunderstanding, I requested: “Can you listen to me please?”, to which “X” replied: “yeh yeh yeh … yeh yeh … yeh yeh …etc”.
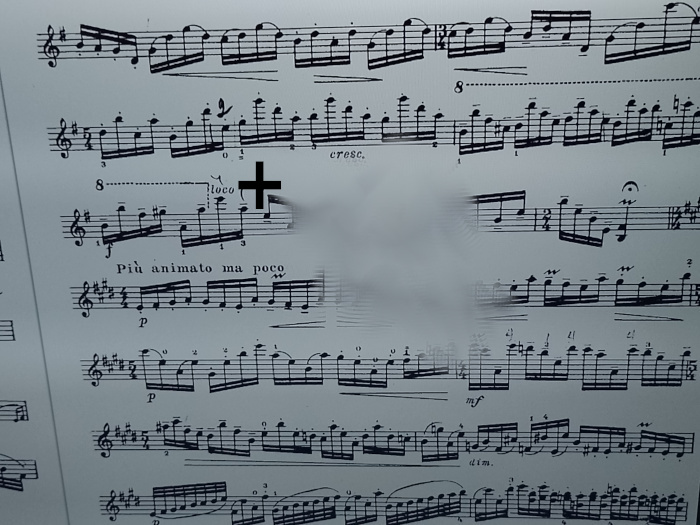
I pointed out what might be a normal distance from a seated position to a music stand. “Yeah I know. At this distance if you want to read the small details of the music you need music glasses” – ‘No. That isn’t the problem …’
At no point during this interview did I claim that I was unable to read “the small details”.
“X” inferred reading ordinary text was no different from reading music.
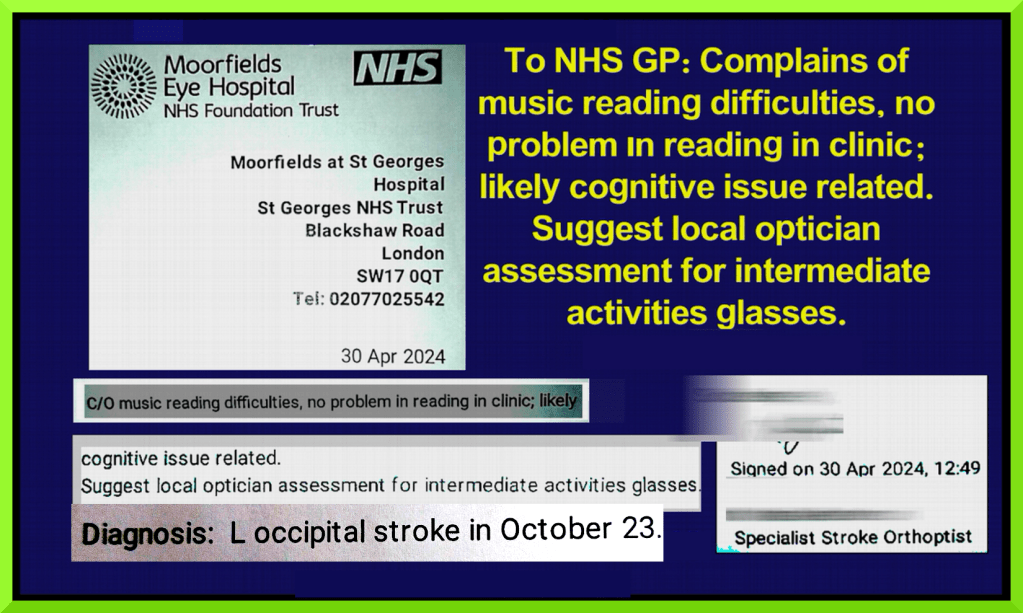
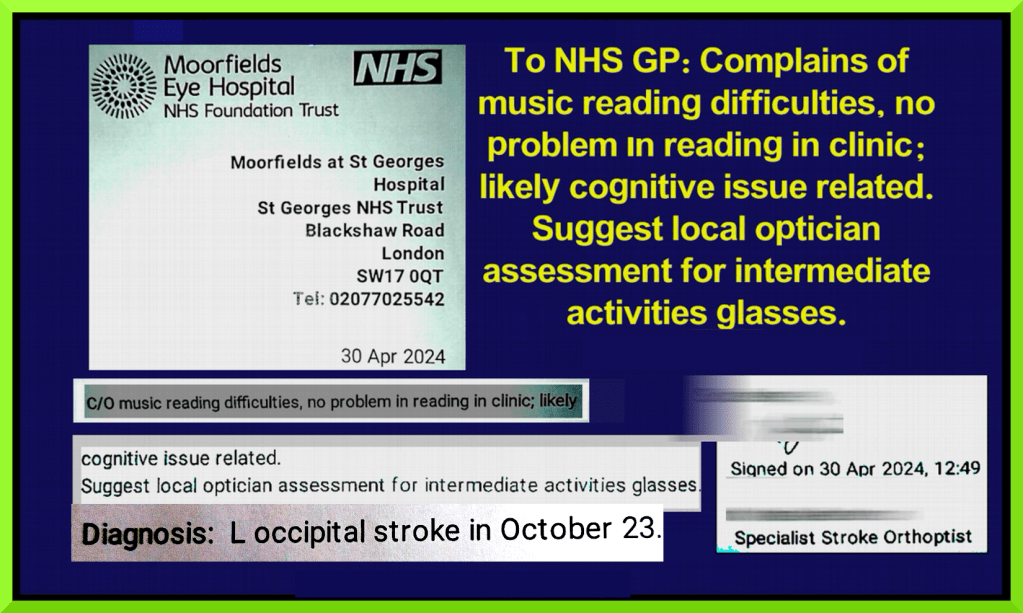
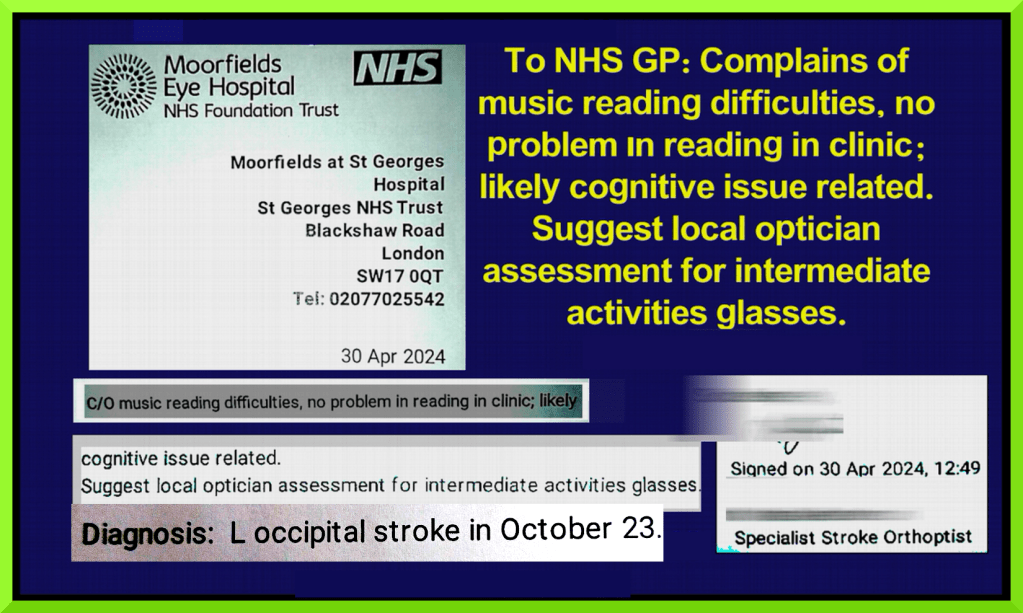
Having then demonstrated I was not able to read ordinary text fluently, I was treated to yet more fallacious rationalisation: “X”: There’s nothing I can do for this slowness, for this speed … You need to move the eyes sir … you read perfectly this line … if you move the eyes … following the line … YOUR VISION IS PERFECT ! … ‘no it’s not’… Angrily: Sir I’m checking your vision now …THIS IS MY JOB! … ‘you must listen to me’ … I objected … etc., and after “X” had further elaborated the complaint (C/O) that I didn’t make, distorting that which I had made clear, i.e. that I can’t see the next bar (etc) to the right because of the central hole in my vision, and twisting it to “Complains of music reading difficulties”, “X” continued to aggressively advance her glasses-as-remedy theory, off the back of her false “C/O” claim, for other NHS personnel, and data analytic systems, and which also misleadingly claimed: “No problem in reading in clinic”.



Among other irregularities, after my second attempt to explain that I couldn’t read text fluently, and being forced to point out ‘I’m not making this up‘, “X” shrieked: “No I do understand. I can understand you are in trouble with the music”, a claim I hadn’t made, there followed two underhand refusals to answer my straightforward question: “What’s the problem when I look at the left hand one and the right one disappears?“


In the interim I decided to go along with “X’s” glasses-as-remedy theory, because I wanted to get away from this disturbing situation as quickly as possible.
Later I was informed that: “The stroke can at times affect the vision but you have no problem at all about vision caused by stroke”. “X” showed me a copy of the Esternman results, destined for an NHS Consultant and my GP Practice … I said ‘but it’s not right’. “X” quipped: “That’s OK you can say it’s not right but this is evidence your vision is perfect“.

I commented that my vision was “OK”, obviously meaning I have never used or felt the need for spectacles, but that it was ‘far from perfect‘.
“X” replied: “That’s OK. If you don’t agree you can go to the local optician and have an eye check to see if you need some glasses“.
[ “eye check” = 12th November 2023 ]
I tried to straighten things out again and gave “X” more examples pertaining to my actual experience.
First up was the disappearing lady, adjacent photos of two ladies on a notice board. I was asked to blink my eyes, to see if the second lady to the right would re-appear, and when that didn’t work “X” enquired: “When does it happen? Does it happen just when you look at the music?” I introduced the disappearing pedestrian, the vanishing dog walker, and the disappearing / reappearing traffic, which sparked off a frantic: “Can you see my finger sir?” slap-dash “examination” by “X”.. and again: “Can you see my finger?”, ‘but your eye’s missing’, “Doesn’t matter”.“Can you see my finger?…Can you see my finger?…how many?” ‘Two’ – The Correct Answer
‘But when I look at your eye, the other one disappears’ … “X”: “OK … In my opinion you are OK“



I repeated that when looking to her right eye, the left eye ‘disappears’, but “X’s” reaction to this was: “OK… In my opinion you are OK. The visual field is perfect” And after mentioning the frustration of missing objects at home, because I can’t see properly, “X” insisted I can see well. “X”: “You can see well sir”. Sounding rather contrived, “X” declared that this was a “cognitive issue, it’s not the vision, it’s something on top of the vision, it’s a cognitive issue, your vision is OK” (‘except it’s not’) “You have the impression it’s not right, but your vision is OK, it’s more a consequence of the stroke“, and “X” explained that this was very common and that it was because of “the damage in the brain and some processes are not like they were before”.

Some considerable time after deciding to ‘accommodate’ “X’s” glasses-as-remedy theory, in order to get away from this toxic situation asap, “X” finally asserted :
“But believe me, visually speaking, you are OK. The stroke has not affected your visual pathway”. “X”: ….. “Does it make sense?” …’Yeah we’ll see…’.
https://en.wikipedia.org/wiki/Quadrantanopia
The only indication that there was anything amiss on the 12th October 2023, was the dramatic and sudden loss of half my visual field, necessitating a visit to the excellent stroke unit at St George’s Hospital, Tooting.
The entire post Esterman visual field test appointment appeared to be a flagrant archetypal example of “changing” facts to fit a theory.

NHS Moorfields dismiss my complaint
26 June 2024 Dr Martin Kuper Chief Executive:
“I write in response to the complaint you raised with Moorfields Eye Hospital.
I am sorry to learn of your concerns and I apologise for the distress you have experienced.
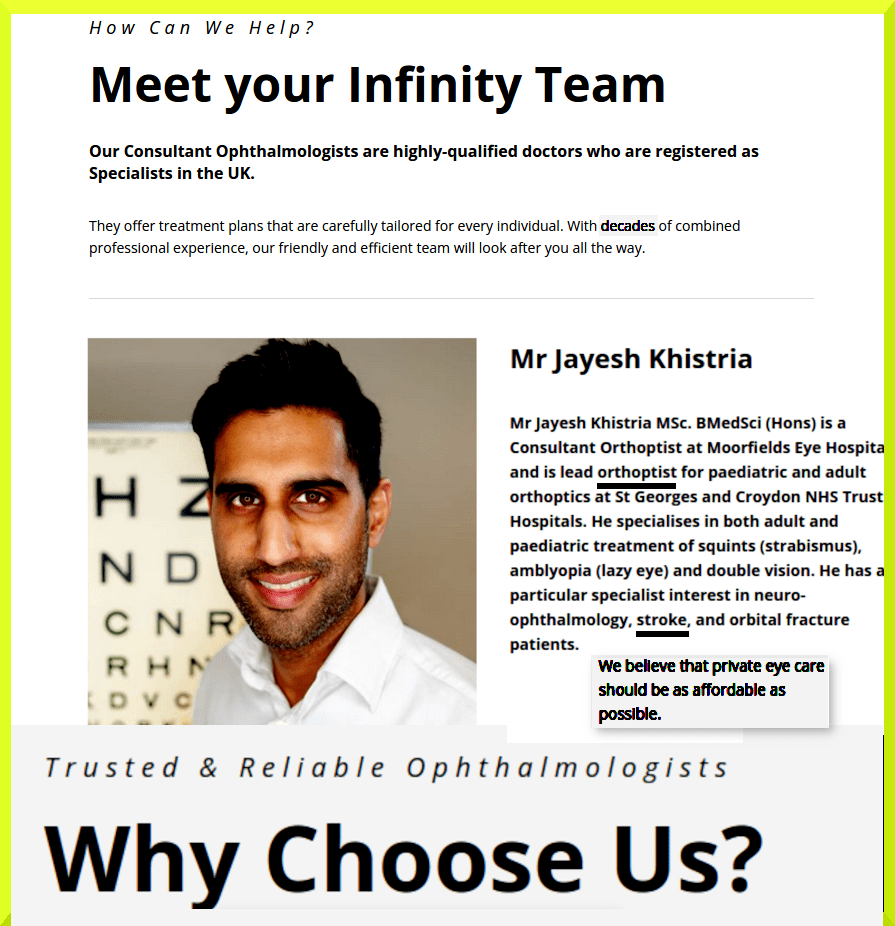
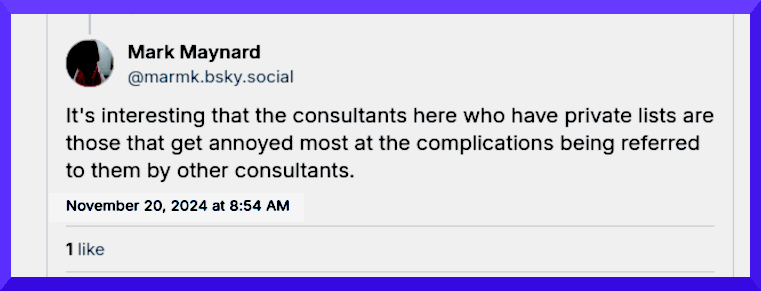
In order to address your concerns, an investigation has been carried out on my behalf by Mr Jayesh Khistria, Consultant Orthoptist Moorfields South who has been assisted by Mr Mark Maynard, Quality Partner Moorfields South.
Following receipt of the concerns raised, Mr Khistria reviewed your medical records, and discussed the consultation you had with “X”, Orthoptist.
Mr Khistria would like to reassure you that following his review of your medical records, he can confirm that a thorough clinical examination was performed, and during your appointment a case history was taken and a measurement of your near and distance vision was taken.
Your vision was recorded as 6/6 in both eyes. A binocular Esterman visual field test was performed which showed that you have full visual fields. The binocular Esterman visual field test is a computerized eye exam that measures your side vision in both eyes together, it is used to assess driving fitness or track vision loss.
An extinction neglect test was also performed this test checks for vision problems where one side of the visual field is missed when both sides are stimulated together. The purpose of the test is to identify visual neglect, a condition where brain injury makes someone miss information on one side of their vision. These tests showed no neglect.
Mr Khistria added that unfortunately it is not uncommon for the objective findings of an examination to not match with the subjective symptoms that patients experience, as happened on this occasion and acknowledges the distress and frustration that this must cause.
“X” has asked me to apologise on her behalf for the distress that you suffered during the appointment and explained that this was not her intent.
Mr Khistria would be happy to arrange for an appointment in a consultant led neuro-ophthalmology clinic so that you could discuss your condition with a consultant, a member of staff from the admin team will be in touch to arrange this for you.
Once again, please allow me to offer my apologies for the distress you have experienced. I hope this letter addresses the issues you have raised; however, should you feel there are aspects of your complaint that have not been adequately addressed, please contact …. Health Service Ombudsman ….. etc.
Yours sincerely
Dr Martin Kuper Chief Executive”
[PDF Properties: Author: haydenc Created Thu 27 Jun 2024 10:34:02, i.e. Mr Chris Hayden, Information Governance Project Manager Moorfields Eye Hospital NHS Foundation Trust]
https://bsky.app/profile/marmk.bsky.social/post/3l33c73n2be2d
[AI Overview] Medical gaslighting—defined as the dismissal, minimization, or invalidation of a patient’s health concerns by healthcare professionals—is a serious patient safety issue where the patient’s subjective reality is challenged, often causing them to doubt their own symptoms
It was ranked as the number one patient safety concern for 2025 by the ECRI, highlighting its role in severe patient harm, including misdiagnosis, delayed treatment, and psychological trauma.
https://en.wikipedia.org/wiki/ECRI_Institute
17th July 2024: “Dear Dr Kuper, Thank you for your letter and apology of 26th June 2024.
In case I have been misunderstood.
On the 12th October 2023 at about 4pm I turned towards the fridge for milk, and on turning back to a kitchen bench, I found half the room had suddenly gone missing. I went to the Stroke Unit at St George’s and was discharged on the 14th October 2023.
Since that point in time, I have had a centrally located hole in my visual field, which has remained constant for over eight months.
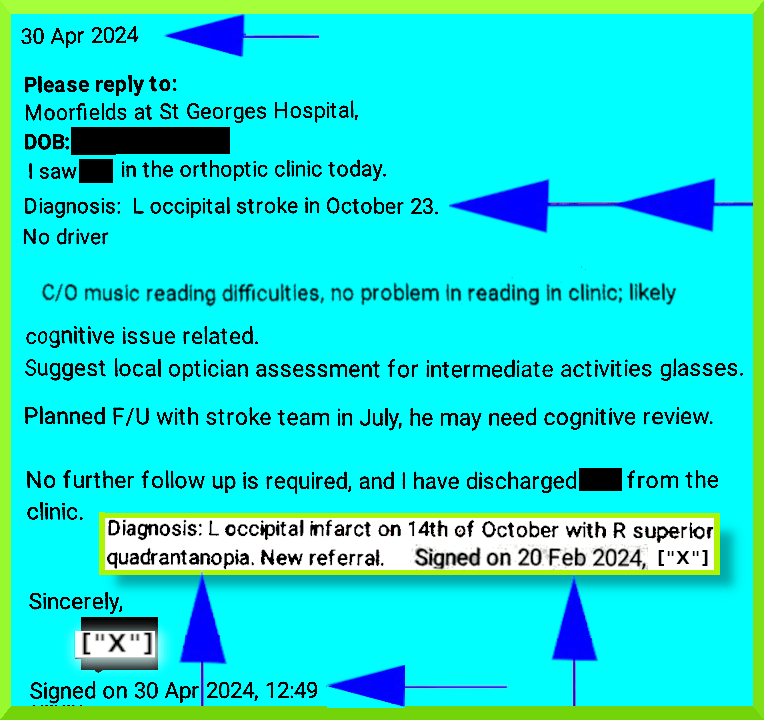
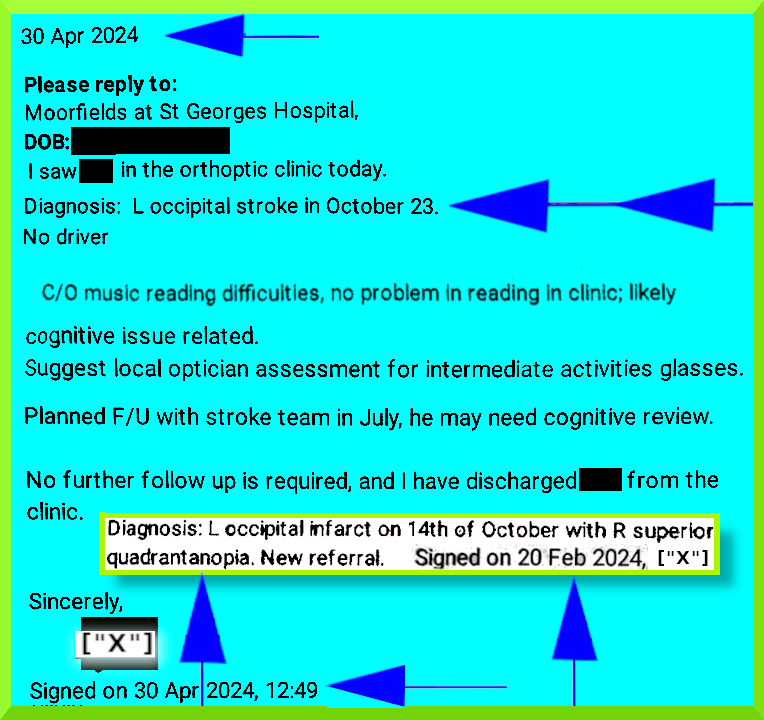
30th April 2024 Moorfields at St George’s (below):
“ … during your appointment a case history was taken and a measurement of your near and distance vision was taken. Your vision was recorded as 6/6 in both eyes. A binocular Esterman visual field test was performed which showed that you have full visual fields. The binocular Esterman visual field test is a computerized eye exam that measures your side vision in both eyes together, it is used to assess driving fitness or track vision loss”
“ ….. showed that you have full visual fields …..”
My centrally situated blind spot interferes with all aspects of my life, in a way that a peripheral blind spot would not.
This includes reading, writing, typing, carrying out precision tasks, kitchen tasks, computer tasks, etc.
When in public spaces, I can miss important facial expressions, cars and bikes can unexpectedly appear/disappear, in busy situations I can collide with other pedestrians, items on supermarket shelves can be difficult to locate, crossing roads can be hazardous etc.
As a consequence of bad experience, I now always wear a discreet body camera when in public spaces, in case of serious collision, or contact with the less than scrupulous.
“Mr Khistria added that unfortunately it is not uncommon for the objective findings of an examination to not match with the subjective symptoms that patients experience, as happened on this occasion and acknowledges the distress and frustration that this must cause”
“ …. objective findings ….”
I maintain that no reliable objective test to identify the centrally situated blind spot in my visual field was carried out.
I was not confronted by the Amsler chart (for example), a grid with central fixation point you can print from the internet, that picks up visual loss quite dramatically.
This might have guided the next investigation, which I presume would not have been Esterman.
The failure of Esterman (“used to assess driving fitness”) to pick up my blind spot, was obvious to me during the test, and I immediately mentioned my suspicion about it to “X” (“it’s in the
middle”, as opposed to periphery) and again later (see Complaint & Addendum below).
“ …. objective findings ….”
“X” carried out several confusing, jerky, subjective and irrelevant office tests, which appeared to be at high risk of operator bias, conscious and unconscious.
“ …. distress and frustration…..”
Nowhere have I asserted that I am experiencing “distress and frustration” because of “objective findings of an examination” that do “not match with the subjective symptoms”, as claimed by Mr Khistria.
“… not uncommon … as happened on this occasion”
What may be “not uncommon … as happened on this occasion“, are other instances of unprofessional careless behaviour, and poor quality investigations, at Moorfields.
It is unacceptable that, rather than immediately seeking help from nearby colleagues in interpreting a test result, when serious doubts are raised, in a hospital clinic setting, the individual concerned (“X”) proceeds instead to systematically undermine my experience and my twice voiced doubts
about test reliability etc.
It is puzzling that Mr Khistria and Mr Maynard did not endeavour to uncover what might have been be driving the imperious, irrational behaviour I encountered at Moorfields at St George’s.
I also complained about the inaccurate NHS Report by “X”, which she intended transmitting to other NHS personnel.
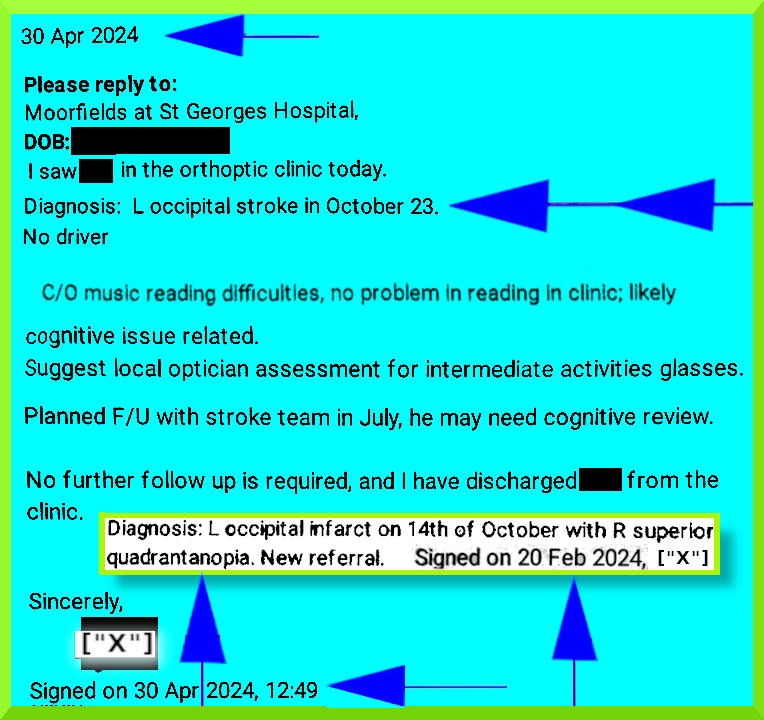
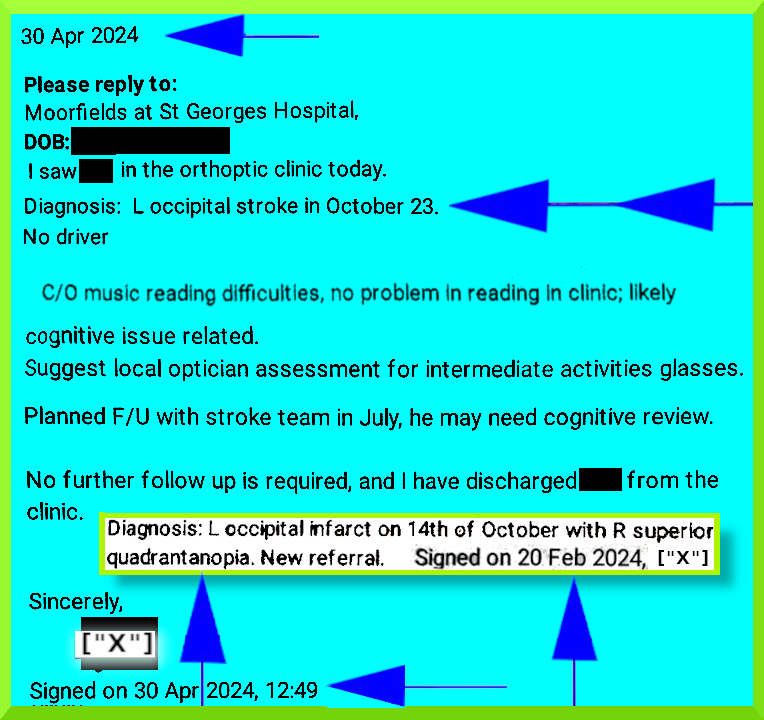
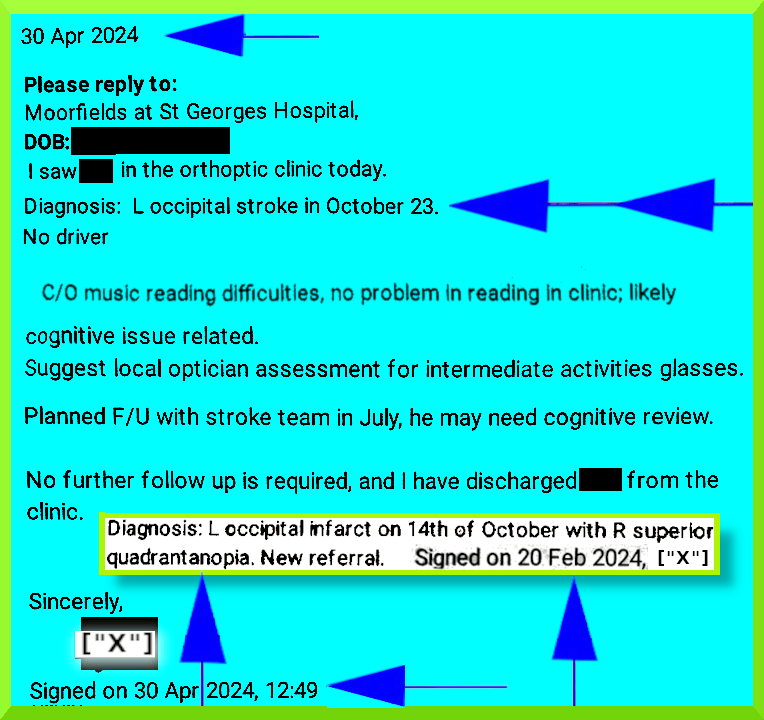
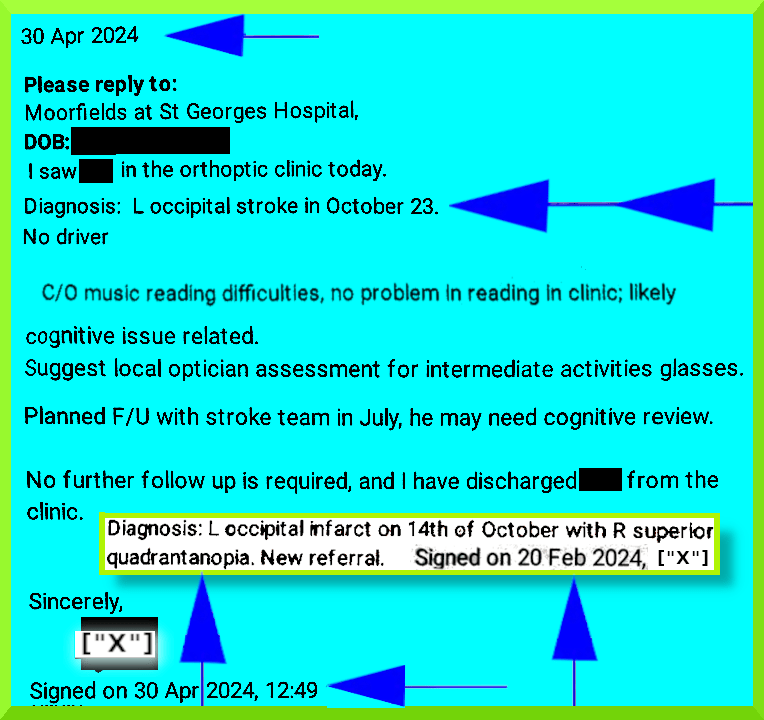
“C/O music reading difficulties, no problem in reading in clinic … cognitive issue…suggest ….activities glasses”
I raised my complaint of (ed. C/O=Complains Of) a subtle but life-altering quadrantanopia about twenty (20) times at my appointment with “X”.
This included flagging up, on multiple occasions, the phenomenon of “disappearing” plugs, eyes, bars (of music), photographs, pedestrians, dog-walkers, traffic, inability to locate objects at home as per usual (mobile phone, earphones, mp3 player, keys, wallet, etc.).
“X” showed no concern for my safety and well-being, and did not warn me about driving, or in my case, using my battery-powered bicycle (just: “Do you drive?” answer: “No”).
My battery-powered pedal-assisted bike has afforded me some level of fitness and freedom, compensating to some extent for my limited mobility etc., which is the result of a disabling illness … <>.
“X” showed no interest or curiosity as to why I was so obviously unwell that day.
“In order to address your concerns, an investigation has been carried out on my behalf by Mr Jayesh Khistria, Consultant Orthoptist Moorfields South who has been assisted by Mr Mark Maynard, Quality Partner Moorfields South”
I had assumed that investigator independence would be a basic requirement, along with an inclusive panel constituted to minimise bias, including at least one disabled individual, who might be better equipped than others to be alert for any signs of exploitation.
I had not received any communication about who was going to be investigating my case, until now.
Obviously, I was unable to discover the expertise, qualifications, values, allegiances, conflicts of interest, evidence of integrity etc., permitting or prohibiting Mr Jayesh Khistria and Mr Mark Maynard to undertake such an investigation, as far as I might have been concerned.
In the interim, I had other matters to attend to away from my home.
I could neither object nor fully consent to this investigation.
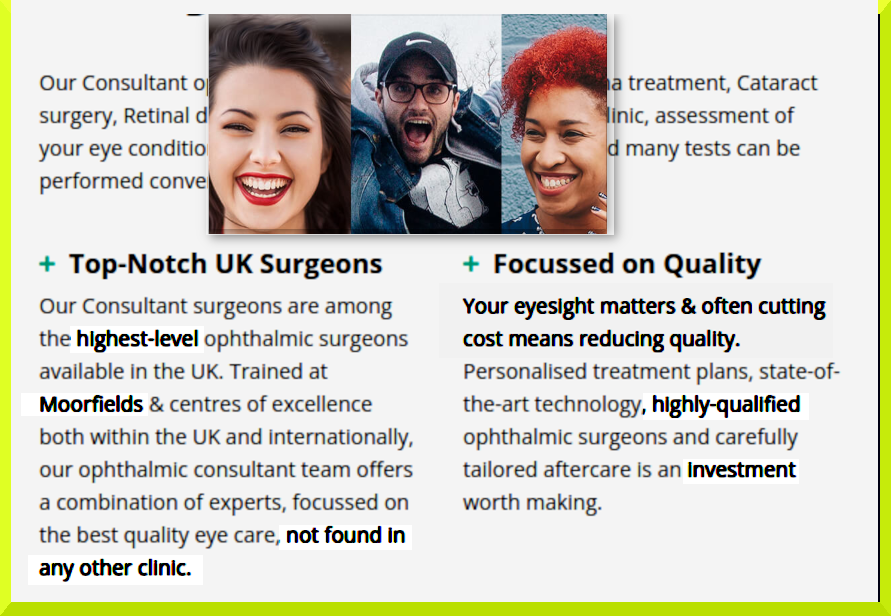
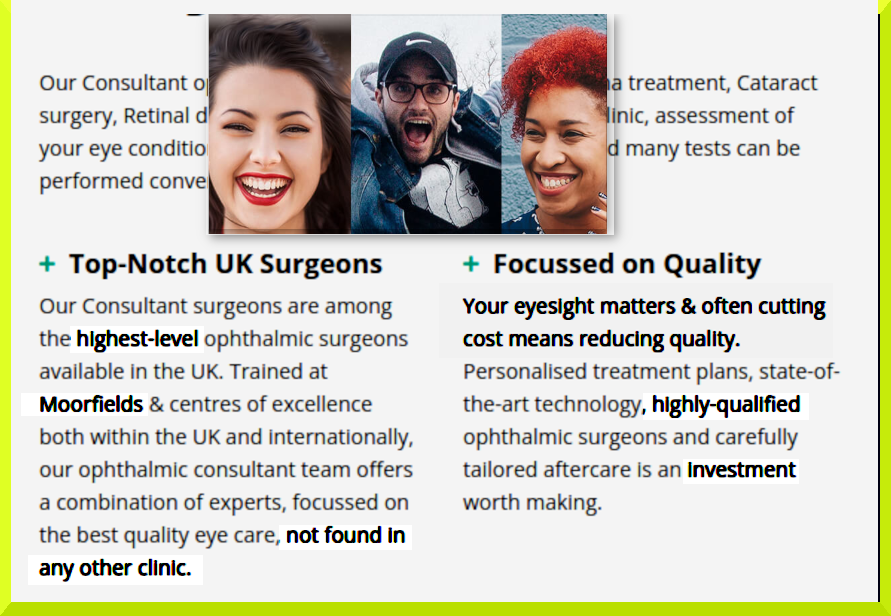
Subsequently, I have found that Mr Khistria promotes himself as “very clever”, “fantastic”, “a very good Orthoptist”, “highly-qualified doctor”, using NHS Moorfields name to attract business at private clinics, while accepting the main role in investigating a complaint against his NHS colleague and friend.
One of these websites uses the lure of “Top-Notch UK Surgeons” to attract customers.
https:// photos.app.goo.gl/
https:// photos.app.goo.gl/
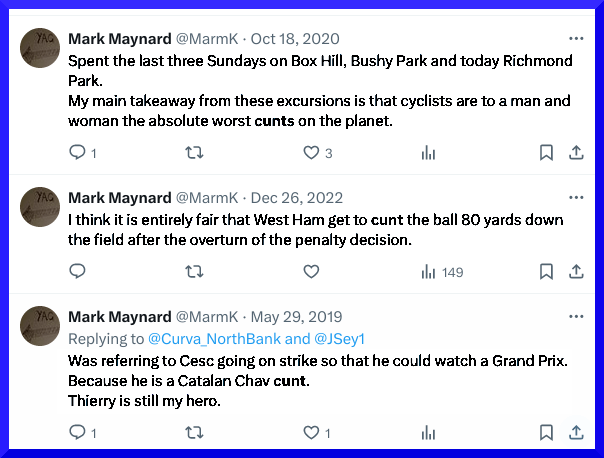
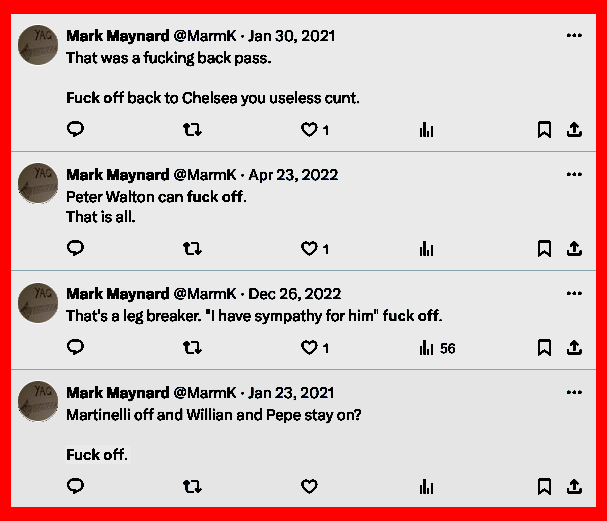
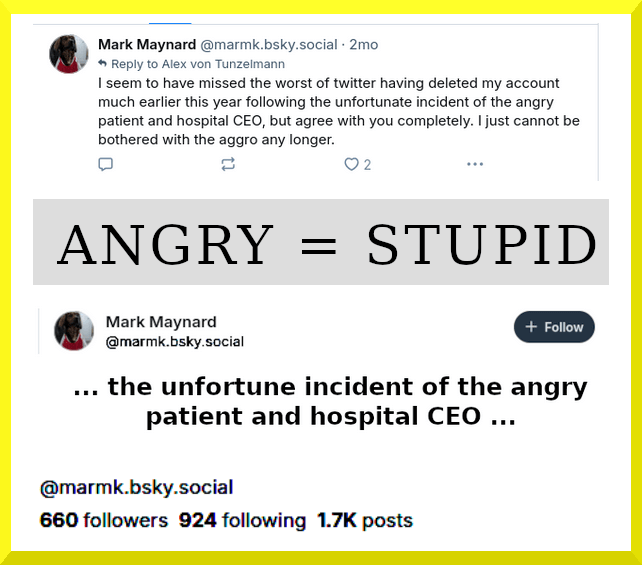
In response to a comment on the day after the tragedy at The Study Preparatory School in Wimbledon, which was the result of a driver’s unexpected epileptic seizure, Mr Mark Maynard
joked on Twitter:
“Jul 7, 2023: I’m sure she had to drive through Richmond Park at least once. That counts as off roading doesn’t it?“
https://x.com/MarmK/status/1677383572280455168
I do not find Mr Mark Maynard’s poor judgement and tasteless joke about a human tragedy, or his misogynist and other offensive language, particularly reassuring.
https:// photos.app.goo.gl/ https:// photos.app.goo.gl/
I do not believe Mr Khistria and Mr Maynard should have had any part in this investigation.
“Mr Khistria would be happy to arrange for an appointment in a consultant led neuro- ophthalmology clinic so that you could discuss your condition with a consultant, a member of staff from the admin team will be in touch to arrange this for you”
“ …. discuss your condition with a consultant …. “
I have no wish to “discuss” my “condition” with anyone at Moorfields.
The lack of any interest in the substance of my complaint in this investigation, is unacceptable.
It does however shine a light on how one might view any offer or apology.
Further, it may reflect a culture at Moorfields, of undermining and dismissing “Complaints” (a valuable mechanism ensuring the health and well-being of your organisation), and one of devaluing and not listening to ‘patients’, as “X” and Khistria lamentably demonstrate.
I wrote in my complaint:
“I believe this needs serious and thoroughly independent investigation, and appropriate remedy”
1) I would be grateful if my request might now be carried out. It may even be in the wider public interest. There could be people out there driving, who shouldn’t be driving.
2) As a matter of urgency and courtesy, I am requesting that “X” write to my named GP, <>, correcting her Report
from:
“C/O music reading difficulties, no problem in reading in clinic … cognitive issue…suggest ….activities glasses” to (for example):
“C/O, being unable to see the right hand object in pairs of objects when viewing the left hand object, in pairs of plugs, eyes, bars (of music), photographs, pedestrians, has difficulty locating objects at home, previously easy to locate, and can miss seeing traffic that is normally in view, and has problems reading in clinic; likely cognitive issue related. Suggest local optician assessment for intermediate activities glasses” (see PS below).
Please copy me in.
3) I would be grateful if you might advise my named GP (above) where I may be referred for accurate diagnosis, and any remedial assistance, and proper support etc., well away from Moorfields.
Many Thanks,
Yours sincerely ……..” [17th July 2024]
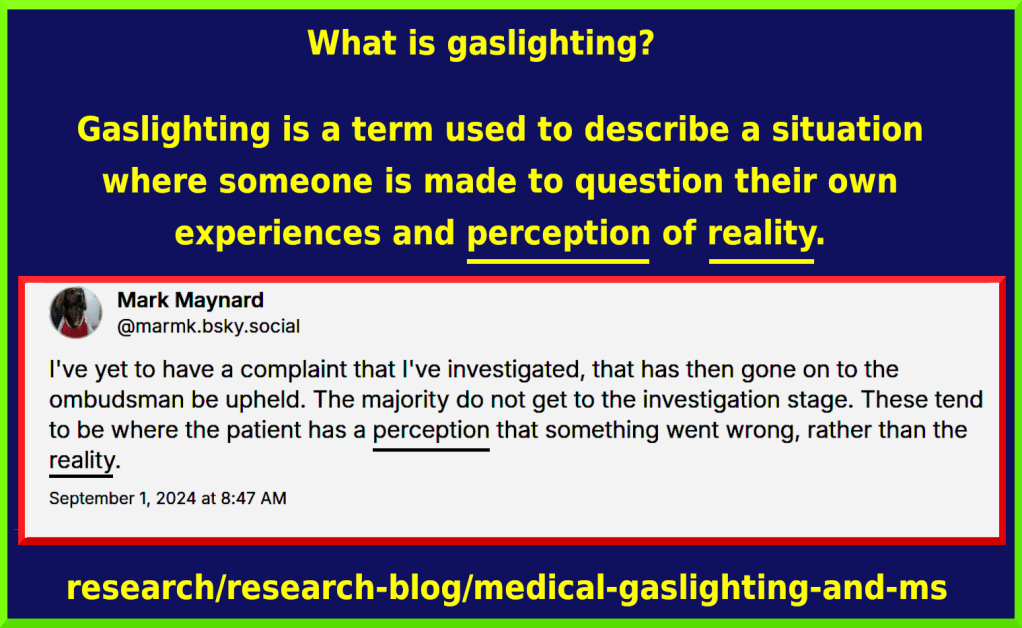
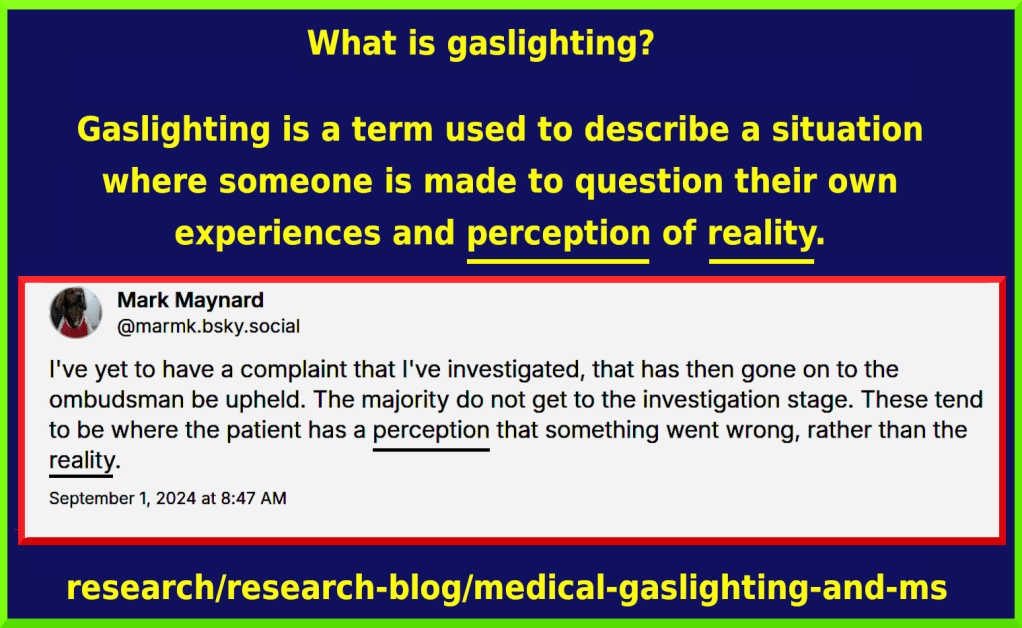
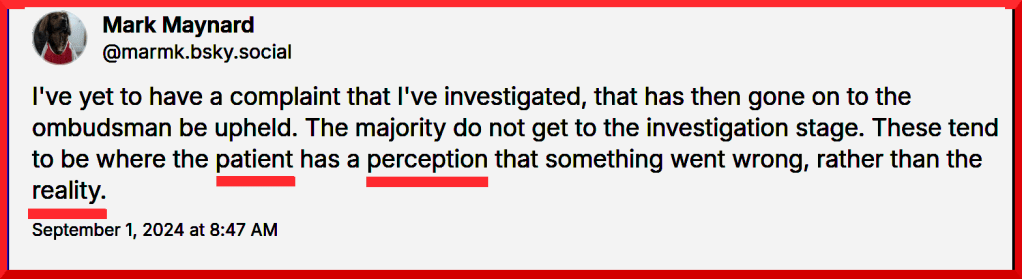
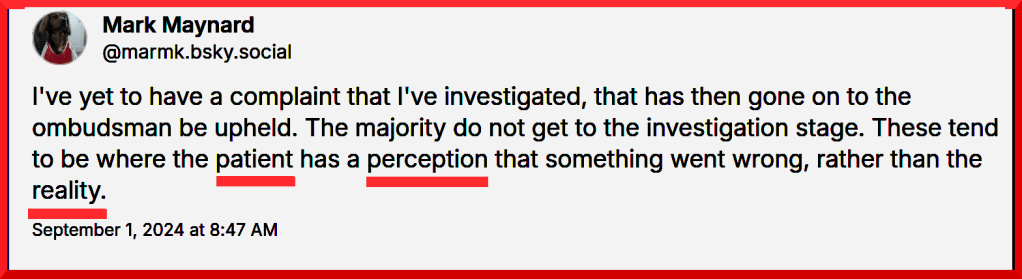
“I’ve yet to have a complaint that I’ve investigated, that has then gone on to the ombudsman be upheld. The majority do not get to the investigation stage.
These tend to be where the patient has a perception that something went wrong, rather than the reality.“
Mr Mark Maynard: September 1st 2024
https://bsky.app/profile/marmk.bsky.social/post/3l33c73n2be2d
Gaslighting is the manipulation of someone into questioning their perception of reality … Medical gaslighting is an informal term that refers to patients having their real symptoms dismissed or downplayed by medical professionals, leading to incorrect or delayed diagnoses; women are more likely to be affected by the phenomenon. https://en.wikipedia.org/wiki/Gaslighting

https://twitter.com/MarmK/status/1677383572280455168
26 Jul 2024 COMPLAINTS (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) wrote: “I understand that “Y” will be contacting you to discuss your complaint and next steps.”
27 Jul 2024 to COMPLAINTS: ” …. Thank you. However, that is quite unacceptable … [Link supplied to “Y’s” “Great to see…” twitter post as one example of two or three implying a potential source of bias, pointing favourably to “X”, plus others, in photos] … “I’m very uncomfortable about this investigation, as indicated in my letter to Dr Martin Kuper. I would like one or more [ed. females on Trust Board I named, before one of them, LWGery, “resigned” ] folks at Moorfields to at least be aware of my complaint the substance of which has been ignored [ed. by three men I would never trust, because of their actions and pompous arrogant false claims about me] … Also I would still be grateful if you might forward me details / membership of the “the division who investigated the complaint” (you mentioned below) … Thus far I have not received a reply from Dr Martin Kuper to my response of 17th July 2024 ….. I should like to know who requested Mr Maynard delete his account, and exactly why his account was deleted? …..etc etc.”



There was no reply to this email, containing straightforward questions, that I sent to Complaints seeking clarification.
30 Jul 2024 “Y” wrote: “Hope this email finds you well. Firstly, I write to apologise that you have had to contact Moorfields twice regarding your appointment on the 30th April, raising concerns about the manner in which your consultation was conducted and with regards to the complaint response. The care you have received is not in keeping the values we uphold and I am sorry that you visual symptoms where not heard or investigated further. I have had a chance to review your medical notes, the youtube video and the other social media you have alerted us to. A formal response will be provided following an internal investigation. I have tried to call a couple of times on the 26th July and today, as I would like the opportunity to discuss this matter further, at a time convenient for you. I understand that trust needs to be earned, and I am committed to rebuilding the confidence you have in our organisation. I do believe your visual symptoms warrant additional investigation and would like to offer a second opinion with the team at Moorfields, at City Road branch where I am based or elsewhere, should you choose. Kind regards, Y“
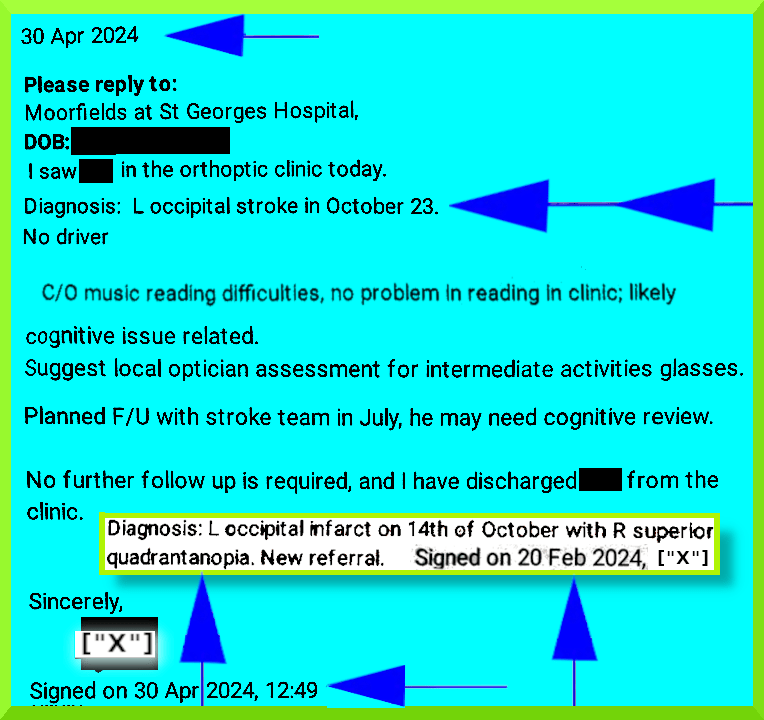
2 Aug 2024: “Dear Dr A [ed. at GP Practice],
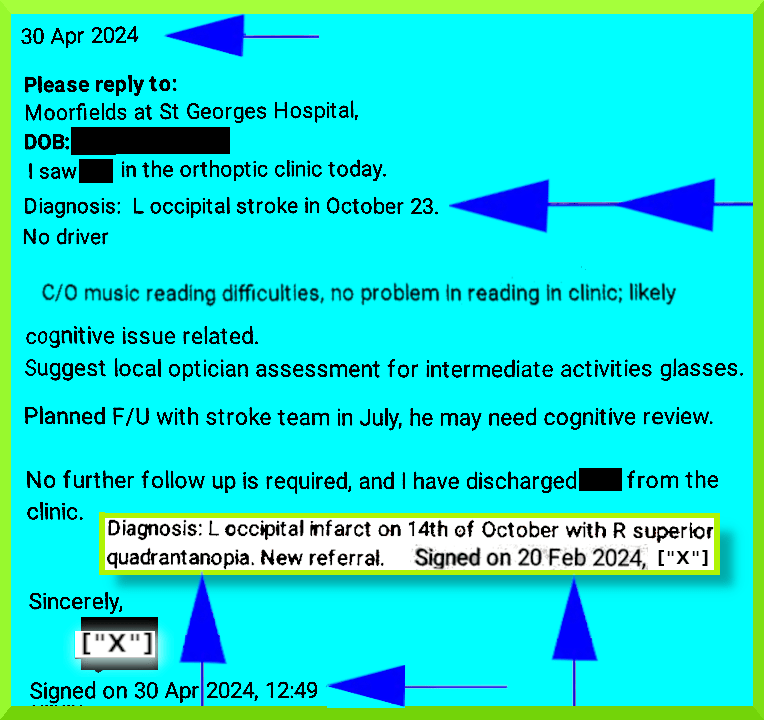
We are writing to advise of an amendment to the letter dated 30th April 2024 from Moorfields Eye Hospital, Orthoptic Service.
Mr ABC continues under our care, and has not been discharged. We have scheduled a follow-up to conduct further ocular imaging, an orthoptic review and consultation with a neuro ophthalmologist relating to his visual symptoms, the cause of which remains undetermined.
Examples of symptoms include:
“being unable to see the right hand object in pairs of objects when viewing the left hand object, in pairs of plugs, eyes, bars (of music), photographs, pedestrians, has difficulty locating
objects at home, previously easy to locate, and can miss seeing traffic that is normally in view, and
has problems reading in clinic”.
Sincerely, Y” [PDF Properties: Creator: PDFium Created:Fri 02 Aug 2024 15:01:37]
https://en.wikipedia.org/wiki/Quadrantanopia
“X” took the liberty of fabricating a complaint I didn’t actually make, which could mislead other NHS personnel about my ability to read and write (etc) fluently, and deny an irreversible situation, putting me at risk in various ways.
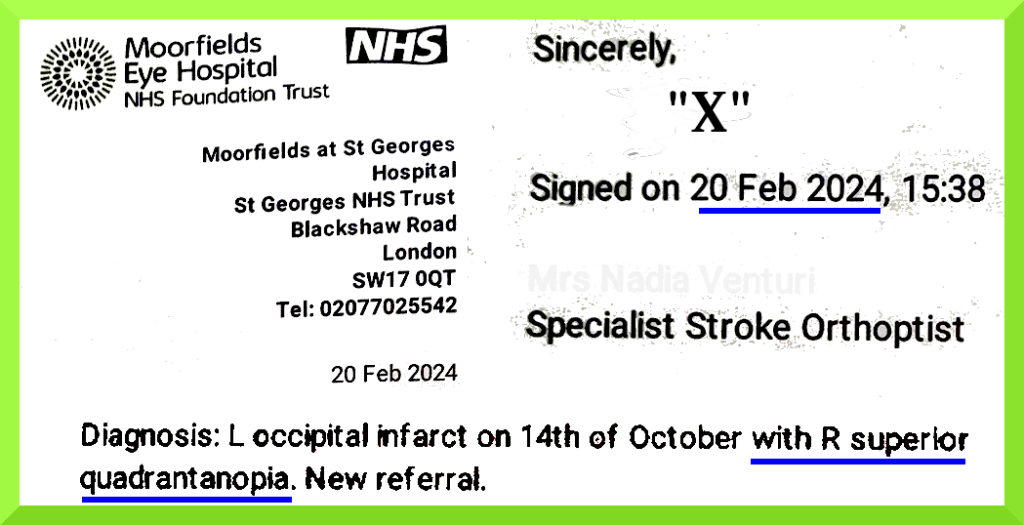
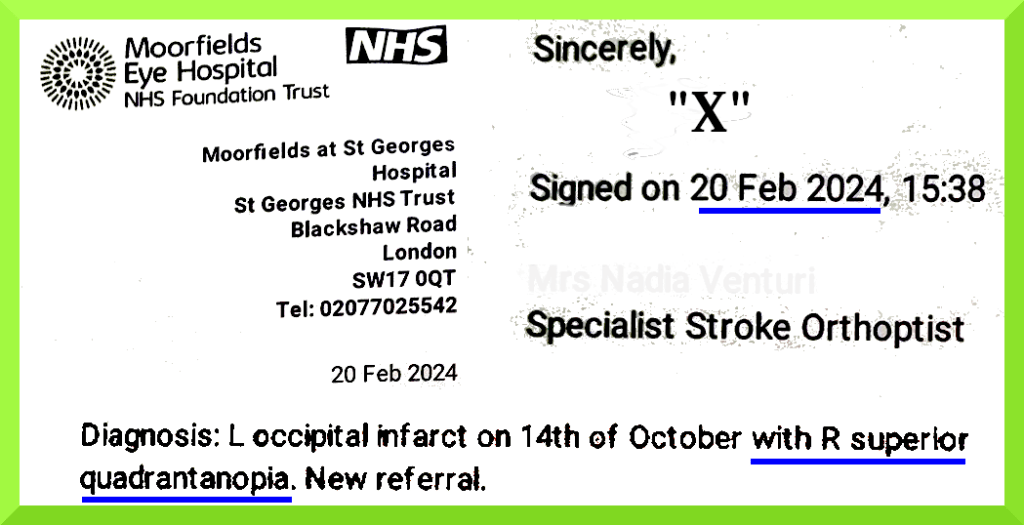
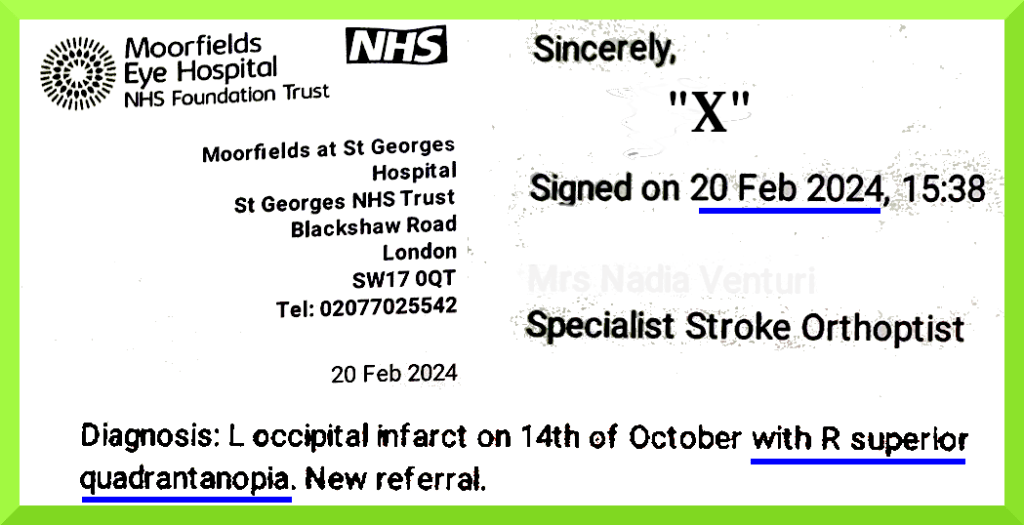
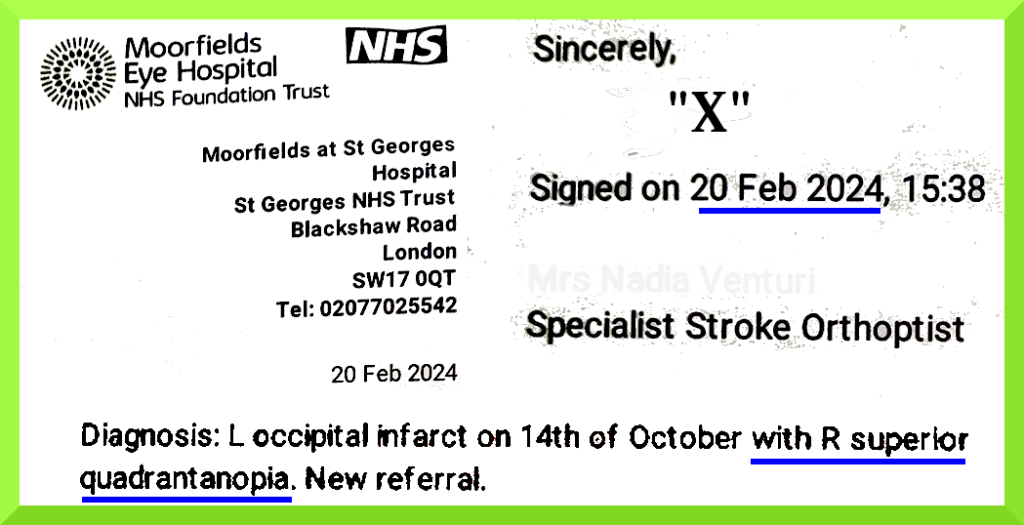
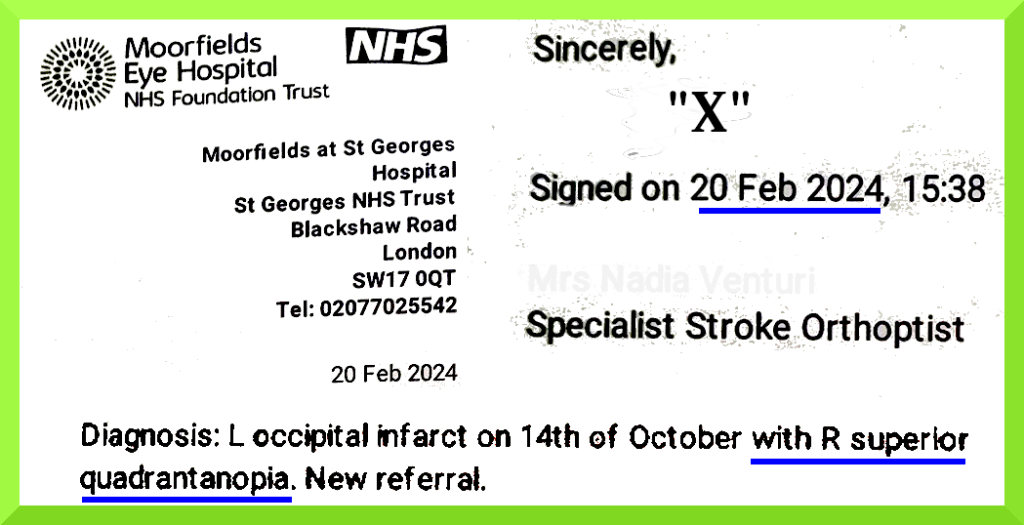
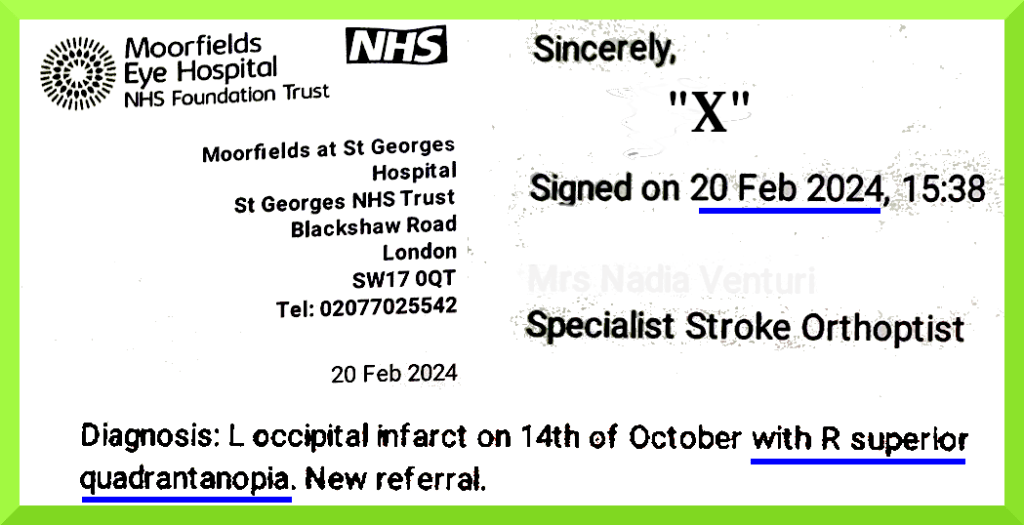
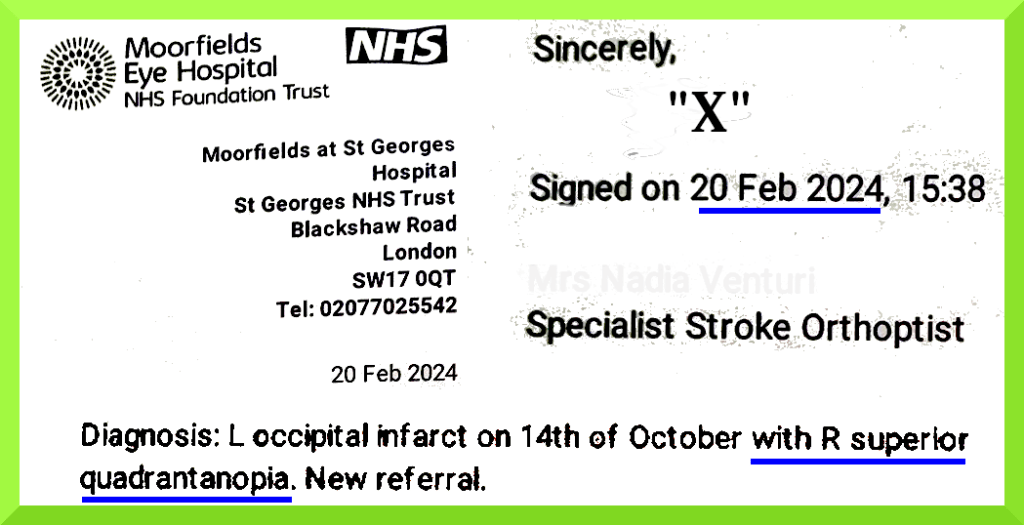
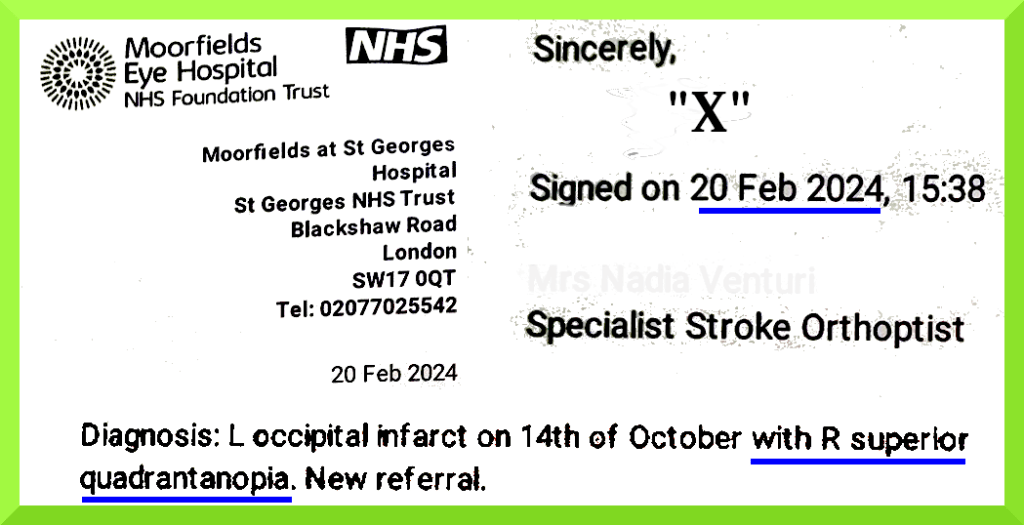
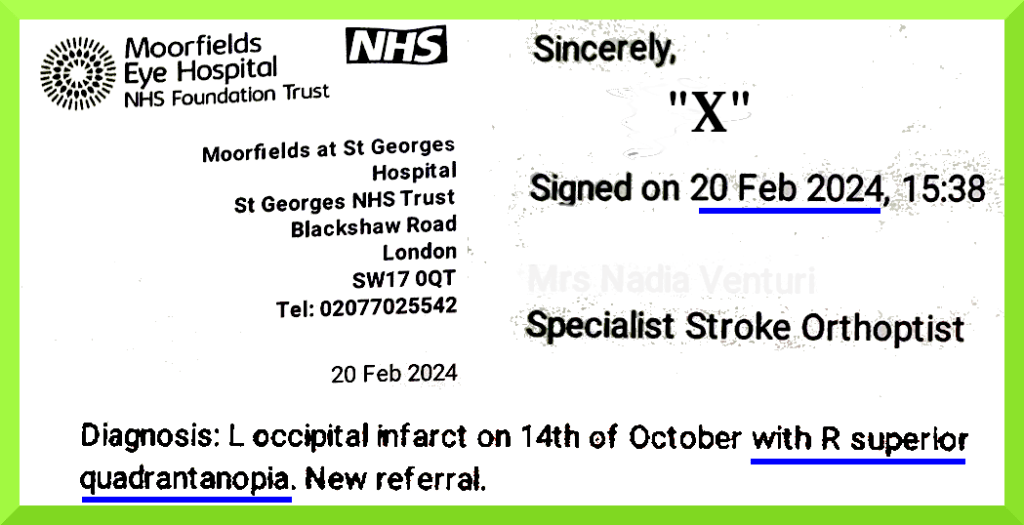
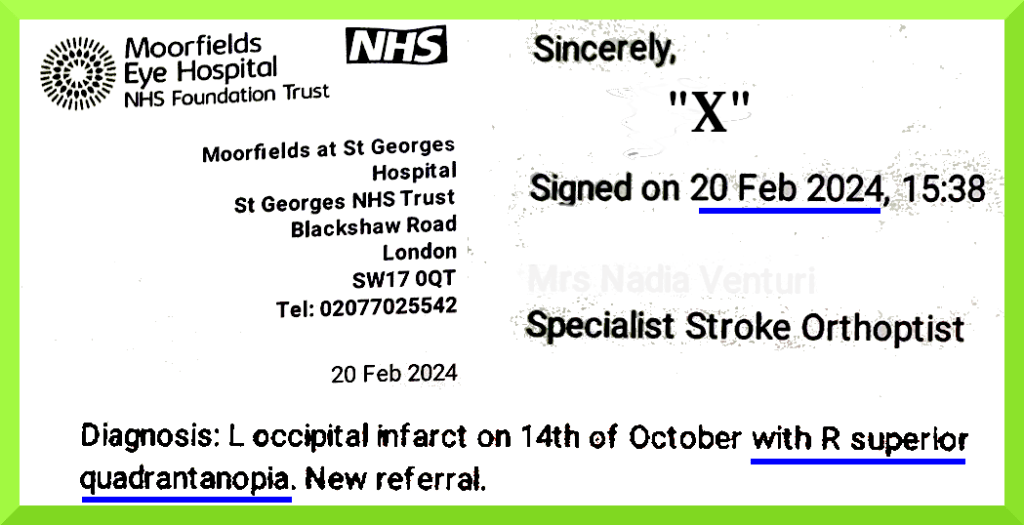
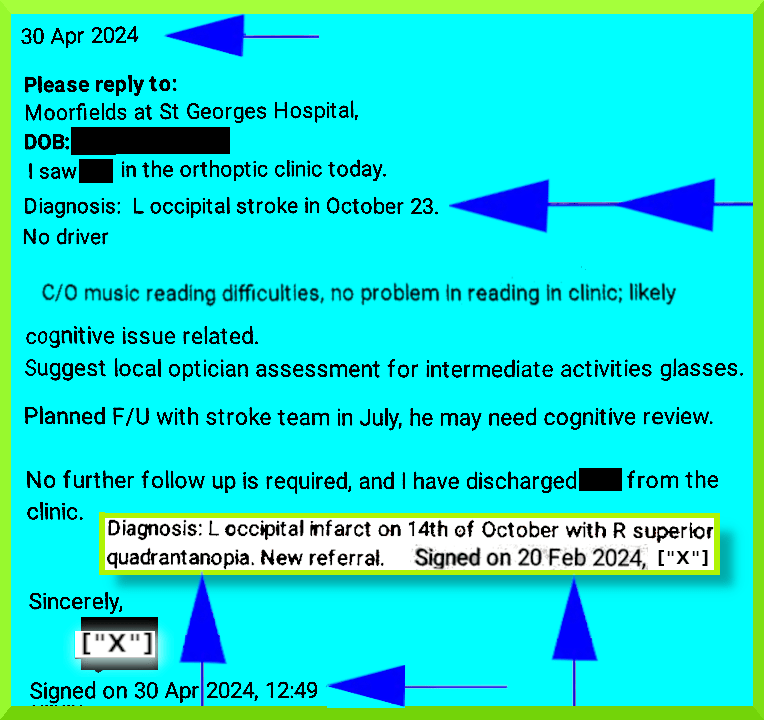
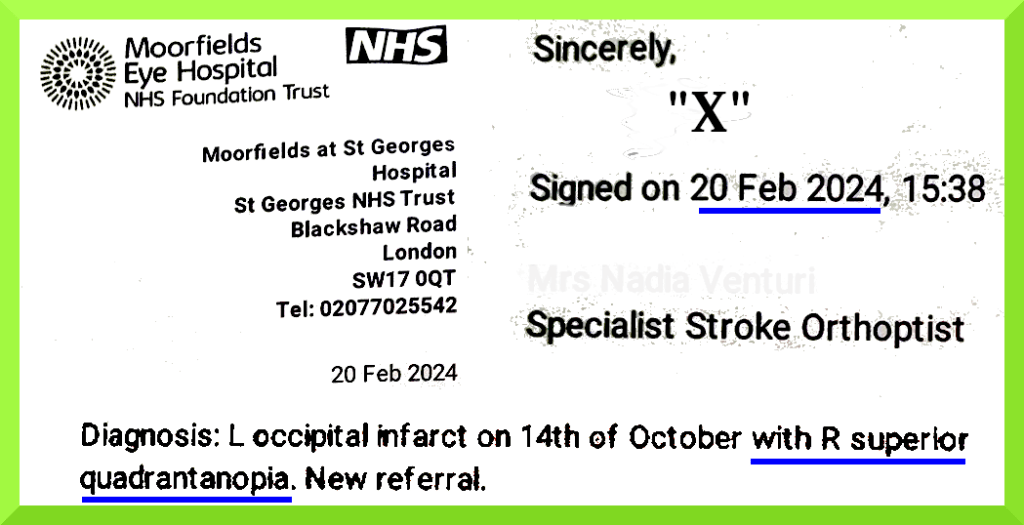
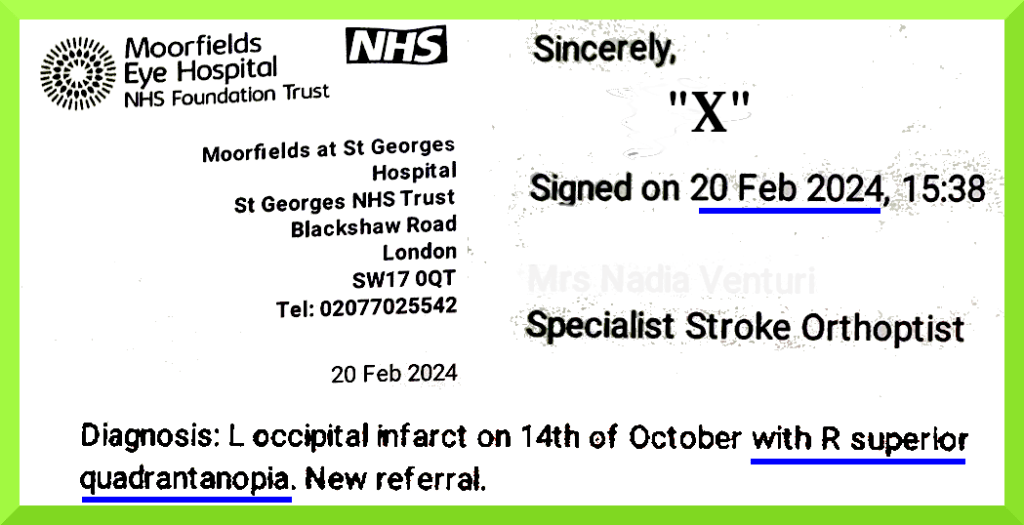
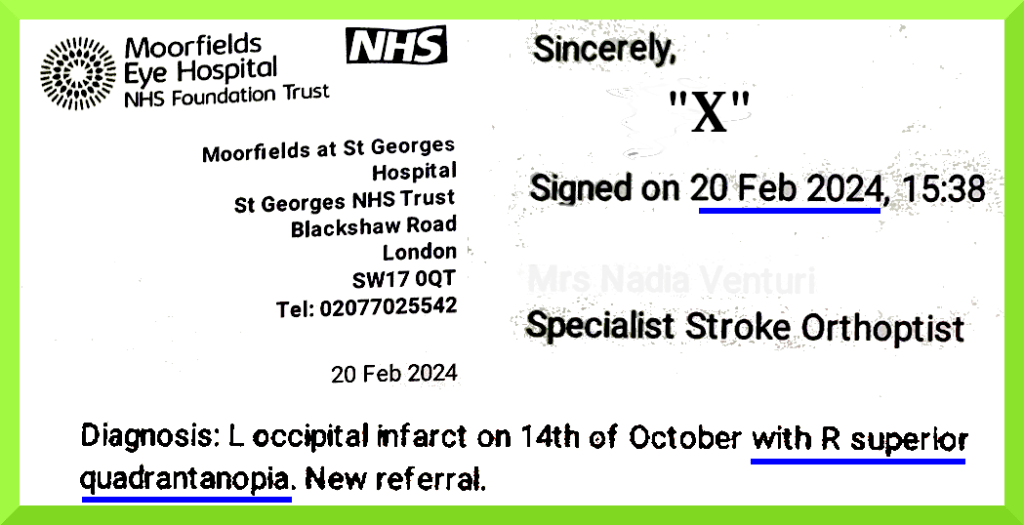
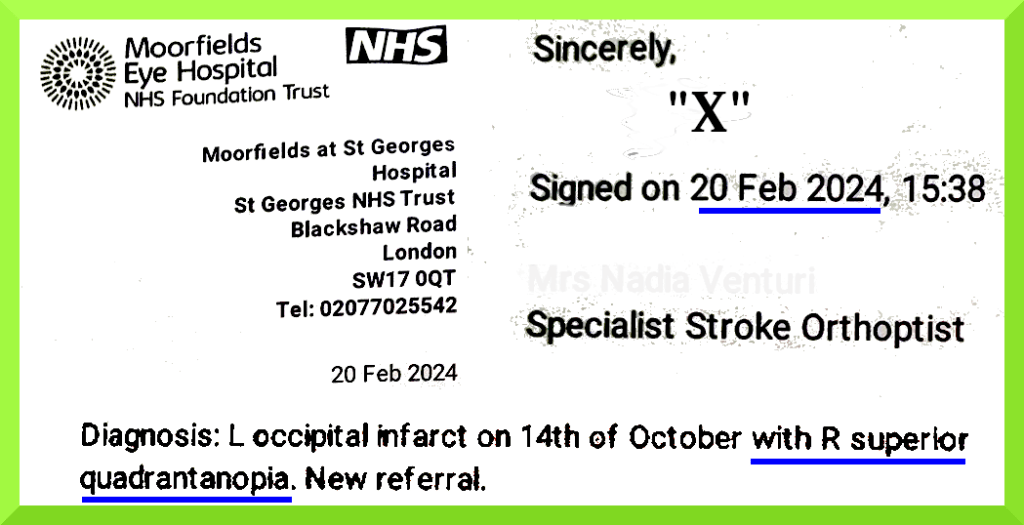
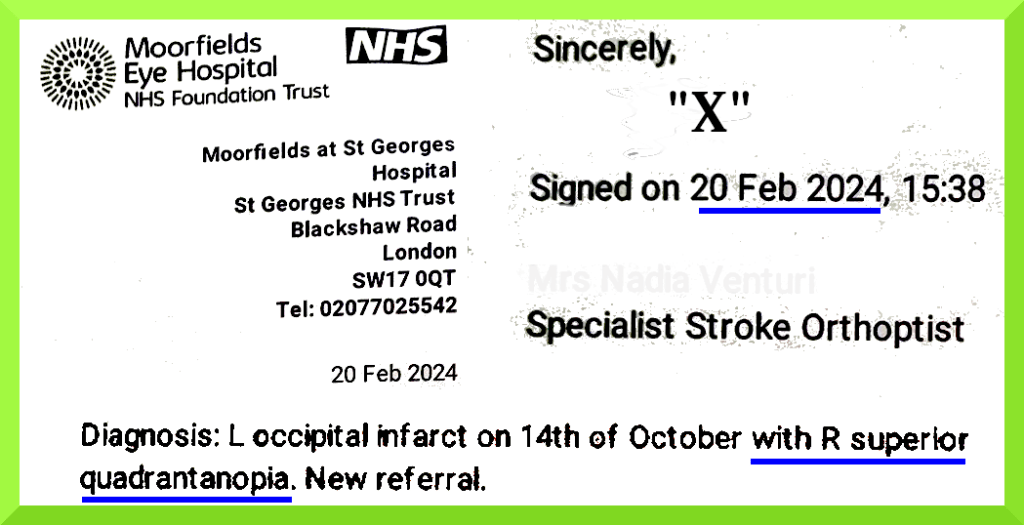
Under “Diagnosis: …”, in her perfunctory report of 30th April 2024, “X” failed to record:
“with R Superior quadrantanopia“, and failed to provide an accurate date (CT 12th Oct 2023, MRI 13th Oct 2023).
During this sinister episode, after I had again suggested that Esterman was “probably not refined enough” , “X” lunged dramatically at the table in front in an effort to swing her computer monitor round, rather inefficiently, so that I couldn’t see what she had been typing (above). Upon setting out to inform me about a possible onward referral , “X” suddenly demanded: “Sir. Are you listening to me? Can you look at me please?”…for no valid reason I could discern. This was part of what appeared to be an attempt to exert control over my attention, away from her computer monitor, with an extended distraction and flurry of activity to try and make sure I couldn’t catch a glimpse of what had been written about me. “X” then continued, “I can maybe refer you to the neuro-opthalmologist and ask them to recheck you. By my opinion, you are OK. …. Your vision is perfect.”

There followed a surly sequence with a stick, the tip of which disappeared because of my blind spot and the angle of gaze. …”You need to follow, sir, with your eyes” (angrily). I attempted to point out that the tip of the stick had disappeared (because of the scotoma) but was drowned out. There was a particularly incongruous: “Well done you’re doing great”… ‘now it disappears’… “Can you follow” snapped “X” at me. There followed a risible rant claiming that for “even me“ (i.e. “X” ), a moving target seemed to disappear if you didn’t follow it, with your eyes: “Do you understand what I mean?”.
“Follow with your eyes …well done … there’s no problem sir, there’s no problem at all”, “X” exclaimed, as if I had no right to be at this appointment, wasting “X’s” time and expertise.

“X” made no referral, and there was probably never any intention of doing so.
Healthwatch: The extent and impact of inaccurate NHS patient records Blog – 1 May 2025: Our latest research found frequent errors in patients’ individual medical records.
“However, coroners have repeatedly issued warnings about inadequate information sharing in the NHS, with some patients dying because clinicians could not access important details about their needs. But is the information in patient records correct in the first place?”
The most common consequence is the inconvenience of filling in the missing information for medical professionals during appointments.
Over one in four (26%) of those who have noticed inaccuracies say they must repeat their patient history, which can be frustrating.
We heard that this frustration is exacerbated by healthcare staff who are not always receptive to patients’ descriptions of their medical history.
Over one in eight (13%) of those who have noticed inaccuracies in their records said they had not received an important test or treatment that they would have if the information had been correct.
A similar number of people (12%) said they had been refused treatment because of inaccurate or missing information.
Concerningly, 10% said they have been given incorrect or inappropriate medication, and 9% said they have received potentially unsafe care or treatment.
The impact of inaccurate medical records extends beyond health care. The information contained in medical records may be used in legal matters, insurance, benefit claims, and other areas.
Over one in eight (13%) of people who have noticed inaccuracies in their record said it has negatively impacted something outside of healthcare.
We heard from someone who encountered issues getting their Personal Independent Payment (PIP) because of missing information in their record.
“A large chunk of my medical records have gone missing. I only found out because I wanted to apply for PIP again as I was turned down a few years before because of lack of evidence. I’ve gone through all the official routes but no one seems to be able to give me an answer.”
https://www.healthwatch.co.uk/blog/2025-05-01/extent-and-impact-inaccurate-nhs-patient-records
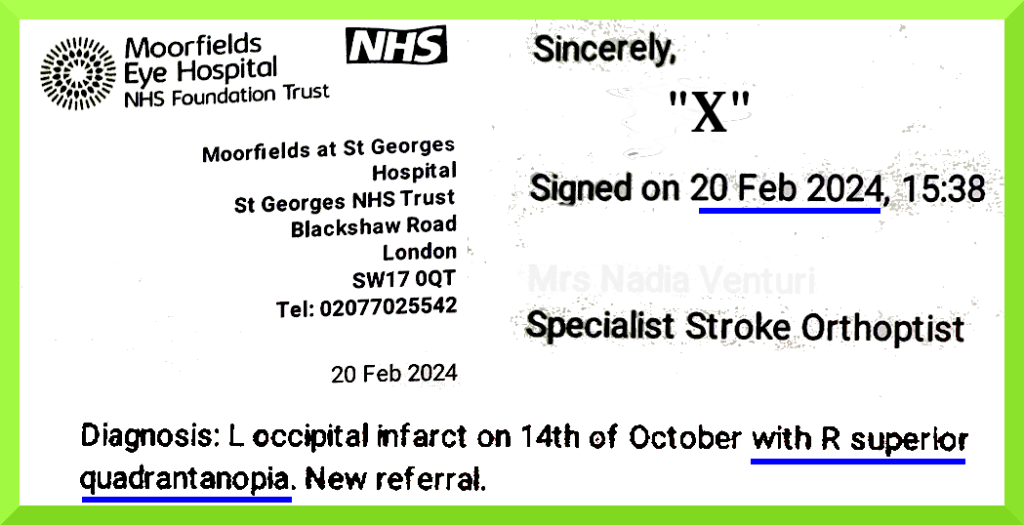
R Superior quadrantanopia omitted at “Diagnosis:” on 30th April 2024
https://www.hcpc-uk.org/standards/standards-of-conduct-performance-and-ethics/
https://en.wikipedia.org/wiki/Health_and_Care_Professions_Council
https://en.wikipedia.org/wiki/Health_and_Care_Professions_Council#Controversy
On 22nd August 2024, in spite of my considerable scepticism, and an awareness of the possibility it might be an attempt to maintain control, I foolishly attended Orthoptics and Neuro Ophthalmology at Moorfields City Road for their “second opinion”.
Apart from discharge letters from both departments, and having heard nothing further from Moorfields, I thought it possible, in view of certain behaviours I’d observed there, that this appointment was a continuation, and a possible face-saving mechanism to somehow get me off their books. In order to cover myself I therefore wrote (1st Sep 2024) an account of my visit to Moorfields City Road, among other details, for the GP Practice, CC’d to “Y”.
1st September 2024 Mr Mark Maynard posted:-
https://bsky.app/profile/marmk.bsky.social/post/3l33c73n2be2d
3rd September 2024 below, posted by Mr Maynard. “ALL THE TIMES = ONE INSTANCE” is my edit.
I supplied about 40 tasteless public posts by Mr Mark Maynard to Moorfields, when objecting to his involvement in my case, amongst which the name Farage occurred in but 2 out of ~40 ‘tweets’ :-

https://web.archive.org/web/20241218015220/https://bsky.app/profile/marmk.bsky.social/post/3l3brhcht7a2e [slow link]
4 Sep 2024: “Y” wrote: “Thank you for cc me in. Hope all is well. Thank you for your patience with Moorfields response, which will include an apology. The letter is currently being drafted and as you and I have discussed I was keen to have the findings from your most recent review to inform on the letter. I did try to call last week to provide an update in terms of timeframe, but unfortunately we missed each other.”
Sidebar
An apology for what ?
On 7th January 2025 I was sent a misleading statement ‘apologising’ that I didn’t receive causal information from the 30th April 2024 Moorfields appointment with orthoptics.
https://en.wikipedia.org/wiki/Orthoptics
The cause of my visual symptoms, established by CT and MRI, had been documented and in my possession since October 14th 2023. This was known to Moorfields on 22nd November 2023, and known to “X” by at least the 20th February 2024.
It was claimed that I had been “seeking assurance around the cause of … visual symptoms”, which was equally offensive and dishonest.
And there was a twisted “apology”, the proffering of which would be beneath the dignity of most reasonably well educated adults.
“I am sorry that you have had cause to complain” Sheila Adam Chief Nurse and Director of Allied Health Professionals
[AI Overview] A victim-blaming apology is a manipulative tactic that shifts accountability away from the wrongdoer by focusing on the victim’s reaction, often using phrases like “I’m sorry you feel that way“. It acts as a defensive deflection, invalidating the victim’s emotions to maintain control and avoid true remorse
This represents the ethical standard of individuals who refer to themselves as “world leaders” and collectively as a “world leading organisation”.
https://www.moorfields.nhs.uk/about-us/join-our-team/our-pillars

Eventually (below), another salaried professional, a Ms Sheila Adam popped up, who appeared to have penned the carefully worded Moorfields Apology within Moorfield’s aforementioned “Formal Response“, “On behalf of Martin Kuper Chief Executive “.
Ms Adam, provided more insight into Moorfields attitude towards the UK ‘NHS’ public.
Presumably not intentionally taking the piss, as far as I could tell, Ms Adam wrote: “I … apologise that the first experience did not provide the information or assurance around the cause of your visual symptoms ….. Once again [sic], I am sorry that you have had cause to complain“.
3 Oct 2024: “Y” wrote: “By way of an update, my report is now complete and your trust response will be with you shortly. Happy to discuss over the phone if you wished.”
5th Oct 2024: ” ….Many thanks for keeping me posted”
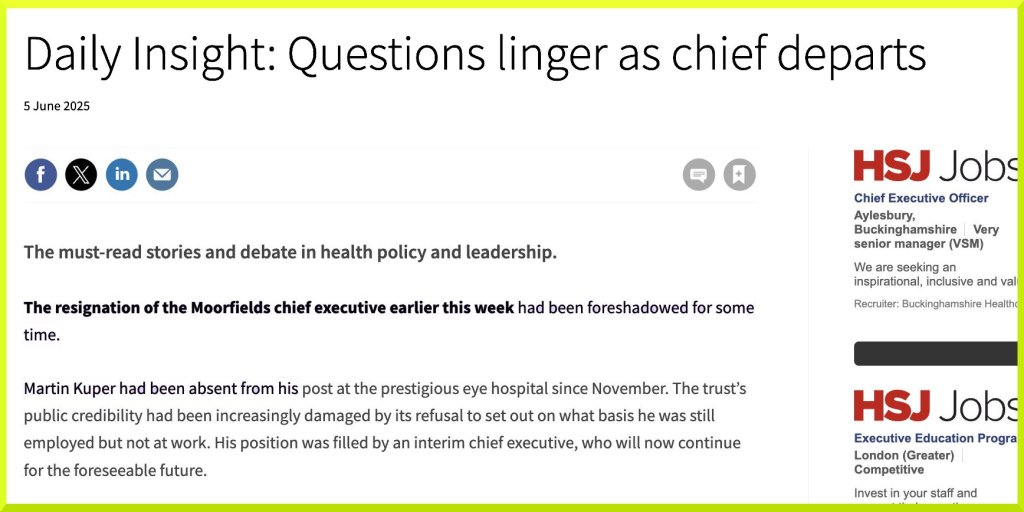
Martin Kuper officially resigned as Chief Executive of Moorfields Eye Hospital NHS Foundation Trust in June 2025, ending a period of significant leadership instability.
Unexplained Absence: His resignation followed a six-month “absence” from his post that began in November 2024. The Trust repeatedly refused to provide an official explanation for this absence.
10th November 2024 Mr Mark Maynard posted:-
https://web.archive.org/web/20250129161828/https://bsky.app/profile/marmk.bsky.social/post/3lalz47ecb62l {slow link]
Board Turmoil: Kuper’s exit was part of a larger exodus of top management. Within a 15-month period, the hospital also lost its chair, deputy chief executive, finance director, HR director, and research director.
Consultant Revolt: In early 2025, more than 80 senior consultants (over half of the hospital’s senior doctors) signed a letter of no confidence in the board.
They alleged a culture of bullying, “coercive behaviour,” and a lack of corporate integrity.
During the period of leadership instability at Moorfields Eye Hospital (2024–2025), the “Freedom to Speak Up” (FTSU) initiative was led by Ian Tombleson, who served as the Lead Freedom to Speak Up Guardian and Director of Quality and Safety.
The FTSU process itself became a point of contention during Martin Kuper’s absence. The 80+ consultants who signed a letter of no confidence in February 2025 explicitly stated they had lost faith in the organization’s FTSU process, alleging it was ineffective in addressing a culture of bullying.
Mark Maynard is a Quality Partner at Moorfields Eye Hospital NHS Foundation Trust. He is specifically responsible for the Moorfields South division, which includes satellite sites like St George’s Hospital, Croydon University Hospital, Queen Mary’s Hospital (Roehampton), Nelson Health Centre (Raynes Park), Parkway Health Centre (New Addington), Purley War Memorial Hospital, Sanderstead Health Centre.
In his role within the Quality and Safety directorate — the same department formerly led by Ian Tombleson — his duties include … Patient Safety & Complaints: Managing the formulation of responses to patient complaints … etc.
[AI responses may include mistakes.]
https://beta.jobs.nhs.uk/candidate/jobadvert/C9273-24-0257
Fri 13 Dec 2024: I updated my GP practice: “The original referral was helpfully arranged by Dr A in mid November 2023 … I was kindly advised by “Y” … that her report regarding an appointment I attended on 22nd August 2024 … had been completed, and that this report along with an apology from Moorfields Trust would be with me shortly. That was over two months ago. Earlier, and without warning or the decency to let me know, Moorfields deleted publicly available evidence I had mentioned to them, which displayed the lack of integrity … [of] Maynard … etc … I trust I shall discover why the report and apology I have been promised has been delayed, without any defensive slant, wasting of other peoples time, or any further shameful waste of precious NHS resources….etc etc.”
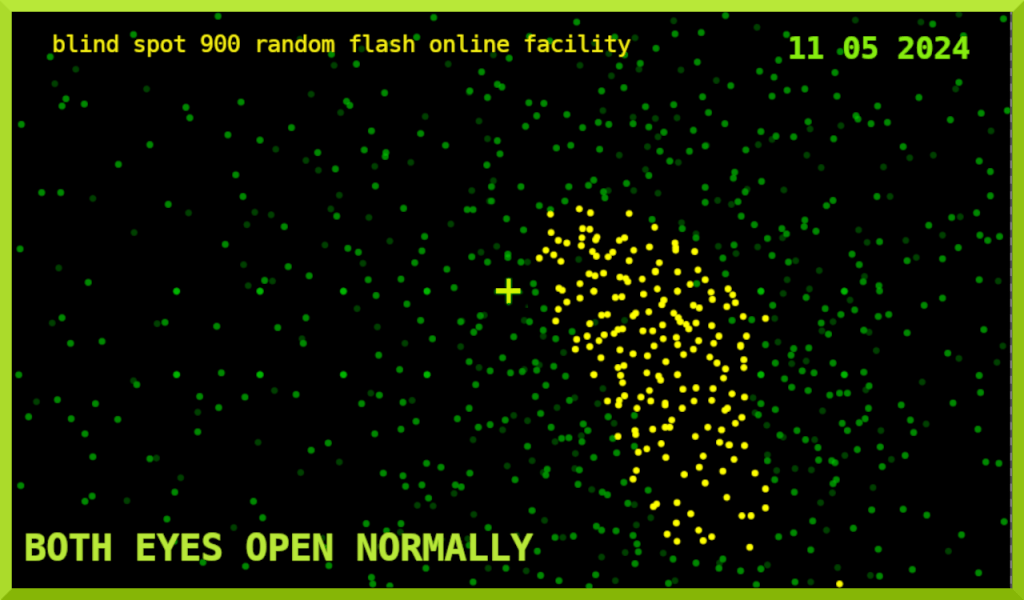
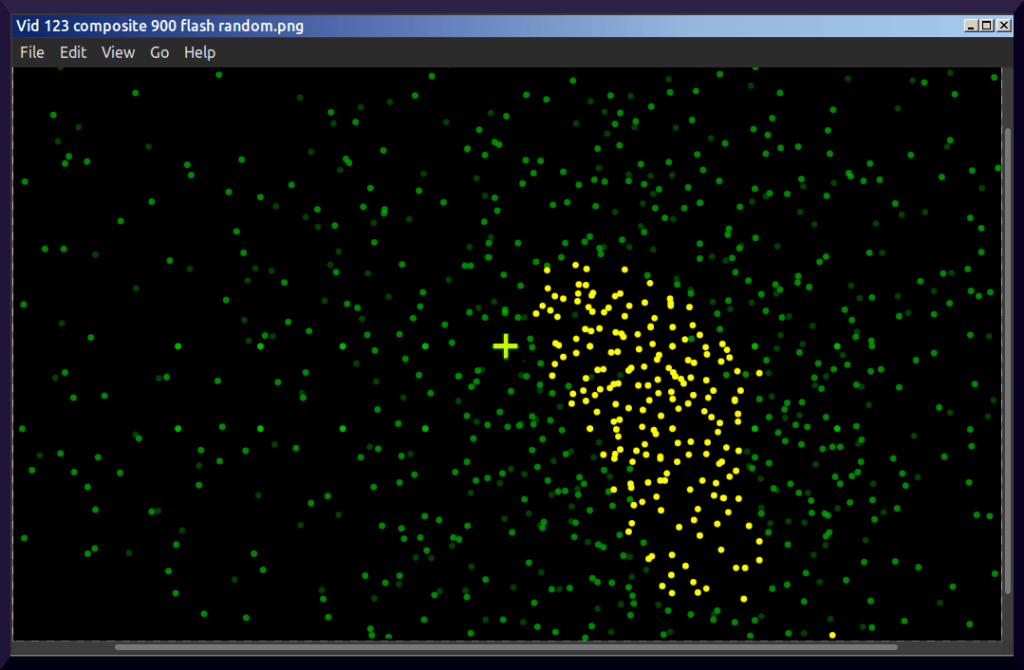
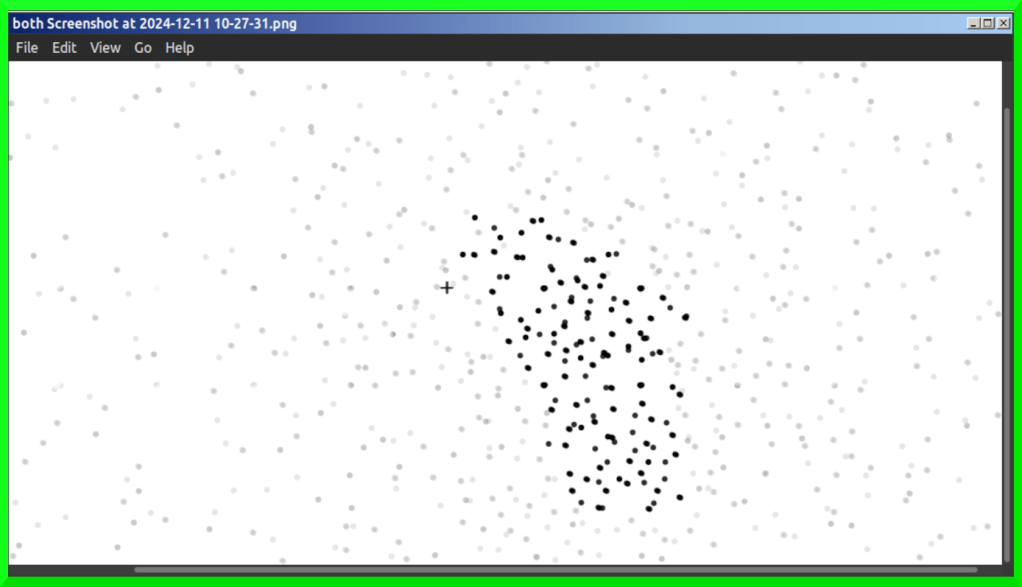
“Below, I shall attach up-to-date read-outs from one of the useful online blind-spot mapping tools. These three separate read-outs (p10) involve ‘left’, ‘right’, and ‘both’ eyes, random flash [x900 per read-out], fixed intensity, and a central fixation point denoted by “+”.
They are a fair representation of my unchanging post-stroke visual deficit (since ~14th Oct 2023), and were produced with the eyes at 30 inches from a 9 x 18 1/2 inch relevant screen area, head on, along the horizontal axis from “+” to the eyes, and which centrally-situated visual field deficit thereby represented, is omnipresent and problematic in many vital areas of life important to me. [CC “Y”] “
11th December 2024: 900 random flash both eyes open :-
13 Dec 2024 “Y” wrote: “Thank you for drawing this to my attention. Let me liaise with the team and come back to you. I am happy to discuss over the phone my findings, if you feel that would be beneficial to provide assurance of the process of improving both the administration, patient engagement and clinic process including communication training.”
In transit – not available until ~ January 6th 2025
7 Jan 2025 COMPLAINTS (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) wrote: “With apologises for the delay, please find attached the Trusts response to your concerns.”
07 January 2025: “Chairman: Laura Wade-Gery Chief Executive: Martin Kuper” on virtual ‘notepaper’.
NHS MOORFIELDS FORMAL RESPONSE AND APLOLOGY
07 January 2025. A Ms Sheila Adam, of whose involvement I was unaware, sent me Moorfields second intellectually offensive “formal response”.
“I apologise for the longer than anticipated delay in responding to your follow- up complaint. Thank you for drawing to our attention your concerns which we have reviewed and would like to outline our findings. We feel there are two elements:
1. The initial consultation regarding the clinical outcome and staff attitude
2. The investigation process itself
To address these an investigation has been carried out on my behalf by “Y”, Dr Z, neuro-ophthalmologist with support from the Central Quality team.
I pleased to hear you have now had a second opinion with Dr Z and apologise that the first experience did not provide the information or assurance around the cause of your visual symptoms. Your GP has also received a copy of the clinical summary [ed. a referral letter] to ensure your medical records correctly reflect that a stroke and not cognitive disorder is the reason for the symptoms described and experienced.
As a result of the follow-on investigation, we have stood up supervision and supported team members to attend internal training and education on communication, to ensure no other patient would have a poor experience as a direct result of a staff members negative behaviour or attitude. The findings from your consultation and the impact of not assessing central visual field has been raised internally and to the professions national stroke team as part of on-going training.
The original investigation missed an opportunity to explore your concerns with professional curiosity, this has been discussed with quality partners, Orthoptic team and divisional lead.
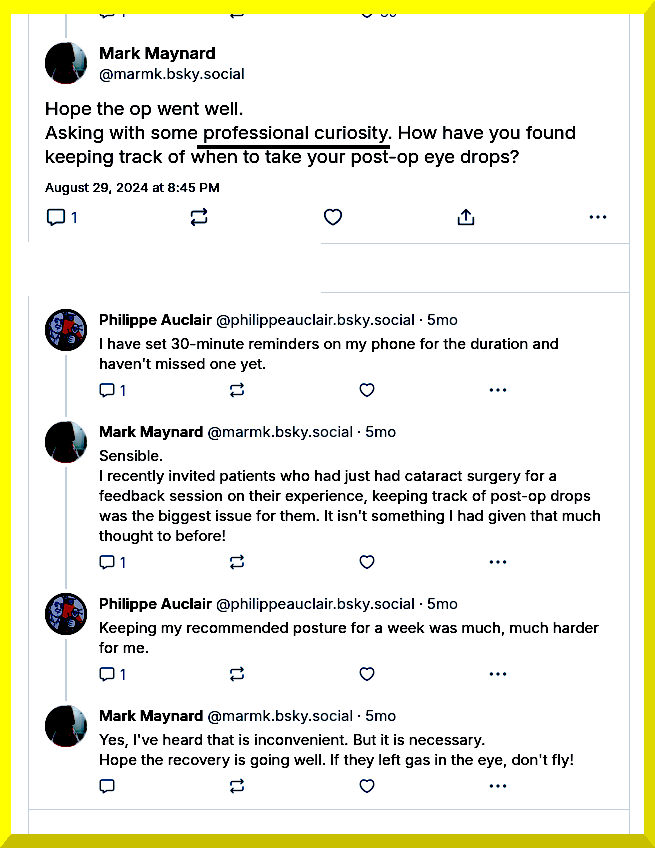
https://bsky.app/profile/marmk.bsky.social/post/3l2uyvykz3b2j
Thank you for taking down the *social media video* and providing us with the opportunity to review the case in its entirety. To help support our response we have provided a summary timeline of each element relating to administration, clinical consultation including follow-up, staff training, lessons learnt and follow-up actions. I hope that we have now been able to address those concerns. I understand “Y”, has a provisional call scheduled to go over the attached document.
Once again, I am sorry that you have had cause to complain and I hope this letter addresses the issues you have raised to your satisfaction; however, should you feel there are aspects of your complaint that have not been adequately addressed, please do not hesitate to contact ….. please contact …. Health Service Ombudsman …. etc Yours sincerely Sheila Adam Chief Nurse and Director of Allied Health Professionals On behalf of Martin Kuper Chief Executive“
Chairman: Laura Wade-Gery Chief Executive: Martin Kuper
http://www.moorfields.nhs.uk [PDF Properties: Author: haydenc Created Tue 07 Jan 2025 10:40:40 ]
haydenc = Mr Chris Hayden, Information Governance Project Manager Moorfields Eye Hospital NHS Foundation Trust
* 07 Jan 2025 “Y” wrote: “Patient kindly stood down you tube video (private link not accessible to the general public – consultation 30.04.2024) “
9 Jan 2025 to: COMPLAINTS (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) “Please could you ensure this letter from Sheila Adam is not sent to anyone else. I shall attend to it as soon as possible….”
10th January 2025 Quick reply under difficult circumstances : “Dear Ms Adam,
Many thanks for your letter and apologies of the 7th January 2025 on behalf of Dr Martin Kuper.
I very much appreciate the enormous amount of work involved.
Although I am sure it’s an oversight, I should be most grateful if you could make it clear that I did not use “social media” as usually understood.
The expression might suggest that I had posted a file publicly.
That was not the case.
Rather, I provided ‘Moorfields’ with strictly private access to an a/v file containing material I had inadvertently collected.
I chose YouTube because it was more convenient and sophisticated than other file sharing methods….”
14 Jan 2025 from“Y” at (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) “Referral letter attached. BWs” “LetterABCAugust2024.pdf” [PDF Properties Author: None Created: Tue 14 Jan 2025 16:11:41 UTC]
14 Jan 2025 “LetterABCAugust2024.pdf” Dated 22August 20 Dr Z wrote: “Please would you offer Mr ABC an appointment in your hemianopia clinic? Diagnosis: post-stroke small paracentral right homonymous hemianopia.
This deficit is causing persisting disability and social embarrassment around the issues it causes, in particular in reading and using screens (the latter being a particular issue e.g. at his local supermarket). There are also practical functional & safety issues – he has also discussed being
unable to see: the right hand object in pairs of objects when viewing the left hand object pairs of plugs or eyes bars of music photographs, pedestrians objects at home, previously easy to locate traffic that is normally in view This was initially misinterpreted as a cognitive issue by orthoptics in the context of only a binocular Estermann field but Mr ABC’s clear history & the Goldmann visual field today confirm the diagnosis. I have attached the visual fields in the hope that they are helpful to Mr ABC as well as to you.
He has looked into many different rehabilitation options but not consistently used any and of course his progress was hindered by this period of diagnostic uncertainty until today. He is keen for referral to see you in your hemianopia clinic, and I have recommended he use the rehabilitation therapy programmes available free online developed by your research labs consistently (at least 30 mins a day at least 5 days a week) to help improve his symptoms.
I have discharged him but would be happy to see again if he would like to be seen in future. We would be grateful if you might offer him a routine appointment with you … etc” [PDF Properties Author: None Created: Tue 14 Jan 2025 16:11:41 UTC]
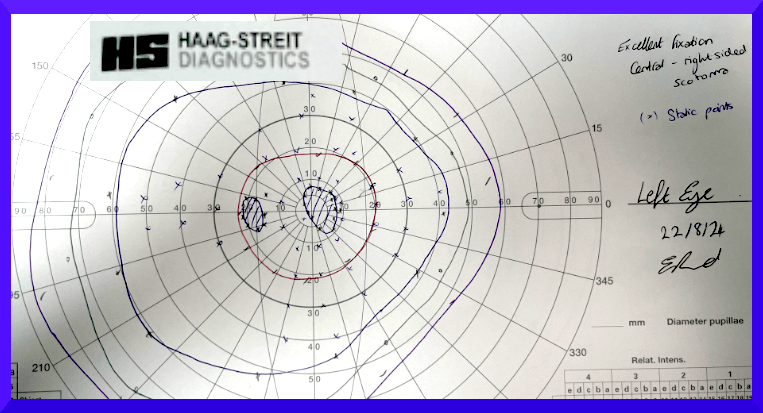
LEFT EYE ONLY

At the above Moorfields City Road “second opinion” appointment on 22nd August 2024, I mentioned a recent experience in an unfamiliar supermarket. I also remarked to Dr Z that a couple of university based online programmes were ‘broken’, and expressed my interest in the work of Aaron Khodami et al.: “we stress the importance of incorporating natural environments, VR, 3D settings, and cognitive interactions to maximize the effectiveness of visual rehabilitation and empower patients to regain their visual abilities in real-world scenarios” :-
“Hemianopia Rehabilitation: From Lab to Life, The Missing Piece” https://www.researchgate.net/publication/371762071_Hemianopia_Rehabilitation_From_Lab_to_Life_The_Missing_Piece
I was informed by Dr Z that it didn’t matter which “mode” was being used.
I did not discuss anything substantial with Dr Z.
However, on 17th July 2024 I wrote to Dr Martin Kuper, then CEO at Moorfields, making it clear that I had: “difficulties with reading, writing, typing, carrying out precision tasks, kitchen tasks, computer tasks, that I can miss important facial expressions, that cars and bikes can unexpectedly appear/disappear, and in busy situations I can collide with other pedestrians, that items on supermarket shelves can be difficult to locate, and that crossing roads can be hazardous.”
And I wrote: “As a matter of urgency and courtesy, I am requesting that “X” write to my named GP, correcting her Report
from:
“C/O music reading difficulties, no problem in reading in clinic … cognitive issue…suggest ….activities glasses” to (for example):
“C/O, being unable to see the right hand object in pairs of objects when viewing the left hand object, in pairs of plugs, eyes, bars (of music), photographs, pedestrians, has difficulty locating objects at home, previously easy to locate, and can miss seeing traffic that is normally in view, and has problems reading in clinic; likely cognitive issue related. Suggest local optician assessment for intermediate activities glasses” (see PS below).
Please copy me in.”
The below impression from May 11 2024 was supplied in “evidence” to Khistria, Maynard, Kuper et al. on 17th July 2024 with eyes 30 inches from 9 x 18 1/2 inch screen area, head on, along the horizontal axis from “+” which represents the fixation point :-

17 Jan 2025 me to “Y”: “I’ve not been able to find [above referral letter from Dr Z] “LetterABCAugust2024.pdf” using online and local mail client searches. One screenshot of email search results is attached, which shows the only occurrence is from 14th Jan 2025 Also for record, I twice emailed Complaints, on 9th and 10th January (c/p below), without receiving a reply. The 10th of Jan was marked high priority and I requested a receipt. I was not aware of the involvement of Ms Adam and I was most concerned about the misleading impression being given by the following (7th Jan): “Thank you for taking down the social media video….” I’m hoping Ms Adam will be able to correct this and reissue her letter.”
17 Jan 2025 me to “Y”: “…. It seems certain I didn’t receive a copy the 22 Aug letter of Dr Z until 14th Jan. I first caught sight of it on the 10th Jan while at an appointment with Dr C at St Georges [Stroke Unit].”
4th February 2025: “Dear Ms Adam, Further to my letter of the 10th January 2025 in response to your letter dated the 7th January, in which you recommended: “I hope this letter addresses the issues you have raised to your satisfaction; however, should you feel there are aspects of your complaint that have not been adequately addressed, please do not hesitate to contact Ms Complaints Manager by email at moorfields complaints at nhs net.”
On the 9th of January 2025 I wrote to Ms Complaints at the above email address ….I remain unsure as to whether or not you have received my letter …. Within my complaint I included, amongst other concerns, the lack of integrity displayed by the Quality Partner, Moorfields South, a Mr Mark Maynard, who supervises Complaints / PALS, and may have access to patient records….
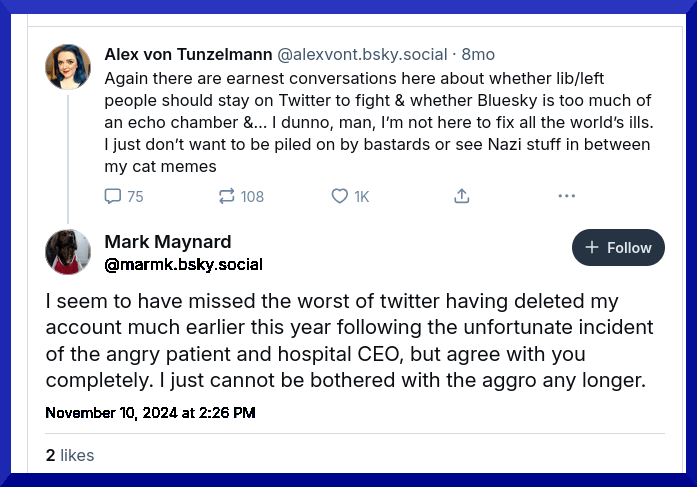
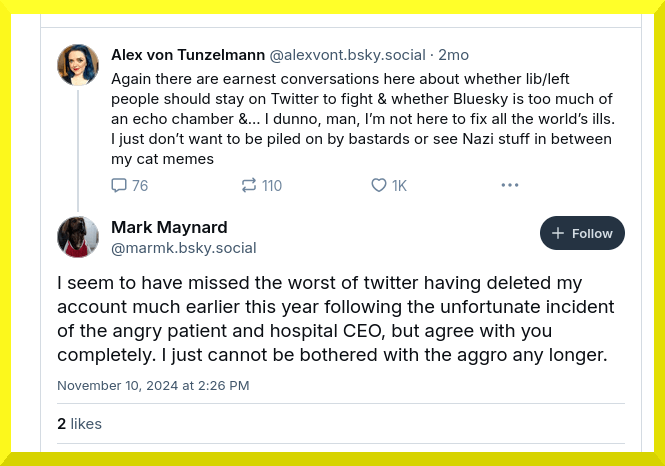
On November the 10th 2024, Mr Maynard registered his contempt for formal mechanisms that help improve the NHS (Complaints/PALS), whilst revealing his contempt for members of the public (patients) engaging with PALS & Complaints, and for Dr Martin Kuper, CEO at Moorfields.
This was publicly signalled on the Social Media Platform Bluesky where his ‘followers’ (500+) can readily deduce which “eye unit” / “clinic” / “CEO” / “hospital” and area wherein he holds the post of “quality manager” where: “It’s a real problem getting access to records for patients…”. This suggests a culture undermining Patients Rights is permitted & tolerated within our NHS ….

https://web.archive.org/web/20250129161828/https://bsky.app/profile/marmk.bsky.social/post/3lalz47ecb62l [slow link]

https://web.archive.org/web/20241218015220/https://bsky.app/profile/marmk.bsky.social/post/3l3brhcht7a2e [slow link]


https://web.archive.org/web/20250129161828/https://bsky.app/profile/marmk.bsky.social/post/3lalz47ecb62l [slow link]
…. Four and a half months later, on the 10th January 2025, I caught sight of a referral letter from Moorfields to Professor C, dated 22nd August 2024, whilst attending an appointment with Dr B , at the Neurology, Stroke, and TIA Service at St Georges Hospital. …. Unaware this document existed, I attended the above 10-01-25 appointment with my own ‘results’ from an online blind-spot mapping tool (p5) …. so that Dr B might get a more accurate picture of my deficit than I am able to detail verbally, and which deficit had been aggressively denied by a “X” of Moorfields …
…. A central issue within my complaint concerned the transmission to NHS personnel of careless, ultimately costly, inaccurate, misleading notes, records, official reports etc., by individuals who have considerable power over other people’s lives …
…… I would be grateful if you could remove references to ‘cause’ & ’reason’ for my centrally situated blind-spot (‘symptoms’) from your letter (p7 below), because that was never at issue (pp10-11)….
Please make it clear that I was exposed to the rude, disrespectful, ageist, loud and aggressive behaviour of “X”, and her dishonest and illegitimate ‘diagnostic’ claims (p12).
I would be glad if you could inform [GP Surgery] in precise detail, that I have made this request, in addition to the other three above.
Thank you for your time and trouble over this matter.
I look forward to hearing from you at your earliest convenience.” [CC “Y”]
5 Feb 2025 Sheila Adam wrote: “I am acknowledging receipt of your email and will respond further once we have reviewed your first and second letter. I have copied in Ian Tombleson, who is Director of Quality and Safety and responsible for the complaints team and process so that he is also aware. Best wishes Sheila ” [CC: “Y” & Ian Tombleson]
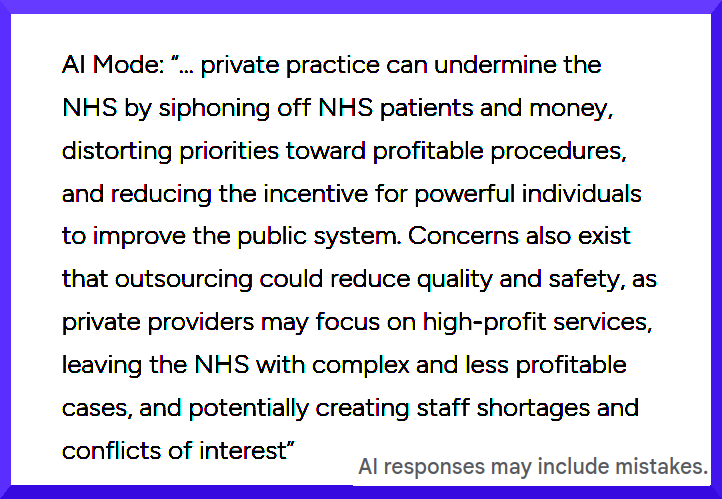
5th February 2025 note to Ms Adam about potential future dangers to members of public resulting from ‘professional’ misinformation, including her own, in connection with dangerous private for-profit ‘data’ companies (4): “Thank you…Where I refer to “this uncertain future”, I include Palantir “buying its way in” to the NHS.” … [ed. with BMJ etc. refs] …. “I did not know who was investigating my complaint, until it was too late ….The stark disconnect between my complaint and the response of Messrs. Maynard and Khistria was troubling … I do think the public should be alerted to any conflict/s of interest in advance, and provided with a statement of personal values and qualifications from individuals tasked with investigating Complaints …”.
Ian Tombleson: formerly of CQC, formerly of Health Service Ombudsman, FTSU Guardian, Healthcare
Management.
* 17.07.2024 Summary Timeline: Social media / private practice of investigators / Social media. This is being managed under
internal processes / 30.04.2024 Clinical appointment. Education and Training / Social media / private practice and team members / managed within internal processes

https://web.archive.org/web/20241218015220/https://bsky.app/profile/marmk.bsky.social/post/3l3brhcht7a2e [slow link]
19 Oct 2025: I wrote to Ms Adam:
“Dear Ms Adam, Further to your reply below of 05/02/2025, I wonder if you have an update as promised. The previous time interval was about six months. Recently I became aware of changes at Moorfields (via HSJ, BMJ etc.), and the context of my complaint therein. After I presented information to you about Mr Mark Maynard’s public discussion of my case, relayed to 32000+ people online, I expect your team will have picked Maynard’s comment (1st September 2024): “I’ve yet to have a complaint that I’ve investigated, that has then gone on to the ombudsman be upheld. The majority do not get to the investigation stage. These tend to be where the patient has a perception that something went wrong, rather than the reality.”
https://bsky.app/profile/marmk.bsky.social/post/3l33c73n2be2d
The implications are disturbing and unacceptable. I had never understood the glaring disconnect between my complaint and the ‘response’*. I did not receive an explanation.
Bragging publicly about how you systematically silence complaints looks like professional misconduct, both the behaviour and the ‘perception vs. reality’ claim, as if people were suddenly delusional.
This is from the same individual who referred publicly to the much younger gentleman, Francesc Fabregas Soler, as “a Catalan Chav c**t”, and who joked online about a tragedy involving children, the day after it’s occurrence, one of whom I understand passed away in the hospital Maynard appeared to be operating from. ….. I have been exposed to abusive and dishonest behaviour. I would appreciate an appropriate and respectful apology, attached to full documentation … Please could you ensure and confirm for me that this email is copied / forwarded to whoever has taken the place of Dr Martin Kuper…”
19 Oct 2025 From: TOMBLESON, Ian (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) CC ADAM, Sheila CC “Y” (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) Many thanks for your detailed email below and links to relevant documents. I confirm receipt. Pleases accept my sincere apologies that you have not received a further reply to your concerns. It is my responsibility to see that your further concerns are addressed. I will liaise with “Y” and we will provide a response to your concerns in line with our processes. Best Wishes Ian
Wed, 22 Oct 2025 from ADAM, Sheila (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST): “Please accept my apologies, I had understood that we would be updating you but clearly this has not yet happened. I know that Ian Tombleson is picking this up on our behalf and has already been in touch.I will leave him to provide a response. Best wishes Sheila. Sheila Adam Chief nurse & Director of allied professionals Director of infection prevention & control Moorfields Eye Hospital NHS Foundation Trust
Mon, 3 Nov 2025 From: TOMBLESON, Ian (MOORFIELDS EYE HOSPITAL NHS FOUNDATION TRUST) “Thank you for your follow up email of 19 October 2025. My apologies again for the extended delay in responding to your queries. In relation to your concerns about clinical correspondence, I have discussed with “Y” and she believes that all relevant correspondence has been sent to you and to GP Surgery. She has said that she is very happy to discuss any further clinical queries directly with you if you would like to email her please (there is no need to copy myself or Sheila into that email).
In relation to your concerns about the social media posts by Mark Maynard, this was addressed as part of a management conversation under Moorfields social media policy and he has removed all inappropriate posts from his social media sites. And as a further piece of information, and to let you know, we have a new Chief Executive, Mr Peter Ridley With best wishes Ian” [Mon, 3 Nov 2025]
It would be interesting to learn from Mr Maynard, and my new friends Sheila and Ian, the precise date when the above and other posts were removed.
Mr Tombleson lifted the veil on Moorfield’s cosmetic approach to reprehensible behaviours.
In view of the standards I’ve encountered at Moorfields, it’s unsurprising that Mr Tombleson ignored my request for a genuine and appropriate apology with complete clinical data all in one document as promised by “Y”, or that he artfully dodged my request: “Please could you ensure and confirm for me that this email is copied/forwarded to whoever has taken the place of Dr Martin Kuper…”



07 Jan 2025: I was advised of changes, improvements, and some actions taken, which included: Patient information leaflets to be readily available from Driver and Vehicle Licensing Agency and The British and Irish Orthoptic Society regarding notifications of symptoms.
* “Y” Summary Timeline, some extracts:-
“No reference would be made to cognitive impairment” [above]
“I finally mentioned to “X” that I lose objects at home because I can’t see properly. This is another very distressing problem. The chilling response from “X” was: “You can see well sir …. it’s a cognitive issue…. you have the impression it’s not right”
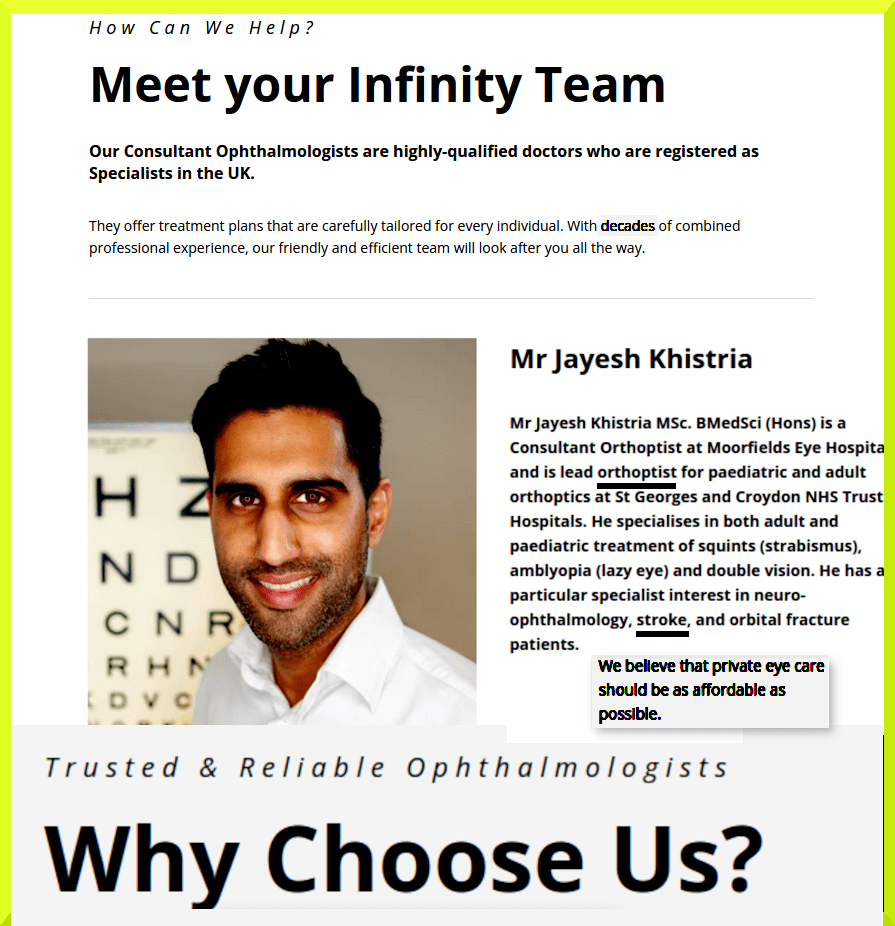
The above collage and other self-promotion:
https://www.infinityeyeclinic.com/team/ https://www.eyesquint.co.uk/

Apart from permanently damaging their integrity, where one act of dishonesty sets in motion a chain reaction, the slippery slope that enables subsequent acts, with the more ambitious further down that variety of career path than others, these are behaviours that impact negatively on UK science, medicine, and society.
My experience could be a common and skillfully concealed occurrence.
The smug, manipulative, devious behaviours and communications, the self-serving excuses (‘misinterpreted’), the deceit of invoking “diagnostic uncertainty”, the lack of appropriate apologies, the manufacture and spreading of misinformation, the lack of accountability and responsibility, the refusal to answer enquiries, the contempt for other people, including wasting their time and their money, which pays NHS employee wages, the striking lack of probity, the patronisng and arrogant attitudes, all of which essentially represent abuses of ‘power’, the nature of which smart organisations, who value other people, wouldn’t tolerate among their employees, and yet which may be the habitual ‘normalised’ standard within our precious NHS, judging from the example of NHS Moorfields.

When the system protects itself: The NHS’s problem with accountability https://www.perspectives.news/single-post/when-the-system-protects-itself-the-nhs-s-problem-with-accountability
“Allegations of professional wrongdoing being quietly ignored is not new in the NHS. For years, senior doctors have been accused of “closing ranks” and protecting one another from scrutiny. Campaigners argue that Martha’s case is not a tragic one-off, but is part of a broader pattern of prioritising the protection of professionals over patient safety. The data suggest this is, sadly, true. The General Medical Council (GMC) finds, on average, 28 doctors guilty of misconduct a year, but evidence from the Patient Safety Watch (PSW) suggests that there may be more than 15,000 “preventable deaths” among people in NHS care each year. The discrepancy between these figures raises difficult questions: are these isolated failures or is there something fundamentally wrong with how the NHS investigates itself, and is there a practical alternative?”
A growing awareness of some aspects of this situation, can be found, for example, in the 2025 Healthwatch report: “The extent and impact of inaccurate NHS patient records Blog – 1 May 2025” https://www.healthwatch.co.uk/blog/2025-05-01/extent-and-impact-inaccurate-nhs-patient-records; “A Pain To Complain” (below) also by Healthwatch ; and “Medical gaslighting as a mechanism for medical trauma: case studies and analysis” (5)
The erosion of trust:
[AI Overview]
Erosion of trust is the gradual decline of confidence in individuals, institutions, or systems, often caused by perceived incompetence, lack of transparency, or ethical failures. This phenomenon weakens social capital, hinders collective action, and impacts sectors like government, business, and health, frequently triggered by misinformation or scandals.
The erosion of trust (3-4), plus pronounced inequalities and poverty in the UK (1), the root of many, if not most “evils”, could at some point contribute to, and help facilitate, power-grabbing by populist “Faragists” (for example, and worse), as happened with Brexit.
“Written complaints in the NHS reached a record high in 2024. With public satisfaction with the NHS at record low levels, the way the NHS handles, responds and learns from complaints is vital.”
” For others, the procedures feel inherently unfair because they see them as
allowing the NHS to ‘mark its own homework‘ “
It would be helpful and in everyone’s interest were there registers available in NHS waiting areas, and online, where members of public can discover the values, relevant interests, affiliations and allegiances, education, track record, private and public incomes, every possible Conflict of Interest, including family connections and conflicts, plus a 1-10 pt. calculation of unequal power differentials, where 10=grotesque, with respect to NHS practitioners with whom the public must interact, and any other relevant NHS employees potentially capable of damaging the lives of others with impunity.
In order to avoid the costly, disgracefully biased and amateurish “complaints” system I’ve stumbled upon, the injustice of which appears to be actively reinforced from within, people ought to know precisely who is investigating their complaint in advance, and exactly what qualifies the investigators forensically and ethically. People should be advised upfront of any possible conflict-of-interest-bias quietly ranged against them, especially if making a complaint involving an NHS organisation with a public reputation about which the CEO’s and others will be highly protective, because of lucrative personal and corporate private enterprise incomes.
https://www.moorfields.nhs.uk/private/locations

https://mediaoffice.ae/en/news/2023/may/29-05/maktoum-bin-mohammed-meets
1] e.g. https://equalitytrust.org.uk/
3] https://www.bmj.com/content/bmj/389/bmj.r1244.full.pdf
4) NHS deal with AI firm Palantir called into question after officials’ concerns revealed Exclusive: in 2025 briefing to Wes Streeting, officials warned reputation of tech firm behind US ICE operations would hinder rollout of data system in England https://www.theguardian.com/society/2026/feb/12/nhs-deal-with-ai-firm-palantir-called-into-question-after-officials-concerns-revealed https://en.wikipedia.org/wiki/Palantir#Controversies In June 2021, reacting to the use of Foundry by NHS, the tech-justice nonprofit Foxglove started a campaign against Palantir because “Their background has generally been in contracts where people are harmed, not healed.” Supporting the campaign, Clive Lewis MP said Palantir had an “appalling track record”.[252] Palantir UK is headed by Louis Mosley, grandson of British fascist leader Oswald Mosley.
AI Overview:
Based on recent reports and 2025–2026 data, Palantir Technologies—often supported by Oracle infrastructure—has become deeply embedded in both the Trump administration’s immigration enforcement (ICE) and military operations in Gaza, drawing intense scrutiny for its role in surveillance and targeting
5) https://link.springer.com/article/10.1007/s12144-024-06935-0 “Being dismissed or disparaged by medical professionals can be shocking and demoralizing for patients, leading to unnecessary harms (e.g., avoidance of medical treatment; depression; shame).” …..
” … The American Journal of Medicine recently published a commentary acknowledging medical gaslighting, stating “gaslighting in medical contexts is often due to the physician’s lack of awareness or understanding of disease entities, preconceived notions about specific clinical presentations, subliminal/unconscious bias toward certain patient populations, or simply arrogance in presuming physician superiority in clinical knowledge and decision-making (Ng et al., 2024, p. 1) … ”
[AI overview]: “Medical gaslighting as a mechanism for medical trauma: case studies and analysis” explores the concept of medical gaslighting and its role in causing medical trauma. Medical gaslighting refers to the phenomenon where healthcare providers manipulate or distort patients’ perceptions of their own experiences, symptoms, or medical conditions, often leading to feelings of confusion, self-doubt, and mistrust.
The paper presents several case studies that illustrate how medical gaslighting can occur in various healthcare settings. These cases involve patients who were dismissed, belittled, or misled by healthcare providers, resulting in delayed or inadequate treatment, and ultimately, significant emotional and psychological distress.
The analysis of these case studies reveals several common themes and mechanisms that contribute to medical gaslighting. These include:
1) Dismissal of patient concerns: Healthcare providers may downplay or dismiss patients’ symptoms or concerns, leading to feelings of invalidation and self-doubt.
2) Minimization of medical errors: Healthcare providers may deny or downplay medical errors, leading to a lack of accountability and transparency.
3) Lack of patient-centered care: Healthcare providers may prioritize their own interests or biases over patients’ needs and concerns, leading to a lack of empathy and understanding
4) Power imbalance: The healthcare provider-patient relationship is often characterized by a power imbalance, with healthcare providers holding more authority and control over patients’ care and treatment.
The paper argues that medical gaslighting can have severe consequences, including:
1) Delayed or inadequate treatment: Medical gaslighting can lead to delayed or inadequate treatment, exacerbating patients’ medical conditions and reducing their quality of life.
2) Emotional and psychological distress: Medical gaslighting can cause significant emotional and psychological distress, including anxiety, depression, and post-traumatic stress disorder (PTSD).
3) Mistrust and avoidance of healthcare: Medical gaslighting can lead to mistrust and avoidance of healthcare, making it more challenging for patients to seek medical care when needed.
The paper concludes by emphasizing the need for healthcare providers to prioritize patient-centered care, empathy, and transparency to prevent medical gaslighting and promote a safe and supportive healthcare environment. It also highlights the importance of recognizing and addressing medical gaslighting as a mechanism for medical trauma, and providing support and resources for patients who have experienced medical gaslighting.
